Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:

YEARLY READERS

NEWSLETTER READERS

FOLLOWERS
YOUTUBE VIEWS
Unlock the Secrets to Effortless IV Cannulation: A Revolutionary Guide for Healthcare Professionals
Explore NYSORA knowledge base for free

YEARLY
READERS
NEWSLETTER
READERS
FOLLOWERS
YOUTUBE VIEWS





Definitive guide to ultrasound-guided peripheral nerve blocks (PNBs) and interventional analgesia injections.
Buy
Guía definitiva de los bloqueos de nervios periféricos (BNP) guiados por ecografía y otras técnicas de analgesia intervencionista.
Comprar ahora!
Guia definitivo para bloqueios de nervos periféricos (PNBs) guiados por ultrassom e injeções de analgesia intervencionista.
Compre agora!




CELEBRATING WORLD BOOK DAY with NYSORA Press 🎉
Despite the rapid pace of digitalization, our research at NYSORA Press reveals that 40% of individuals still prefer the tactile pleasure of physical books over e-books or digital formats.
At NYSORA Press we’re about creating bestsellers! Our titles in Nerve Block and IV Access have already topped Amazon charts, and we’re excited to announce that by the end of 2024, we’ll be adding 10 new books to our portfolio. These upcoming titles are penned by leading authors in the fields of Anesthesiology, Pain Management, MSK, PAIN, POCUS, and Emergency Medicine.
Why do top authors choose to publish with us? It’s simple: NYSORA offers unparalleled support with content development, including innovative illustrations, animations, and videos. Plus, our community of over 500,000 followers ensures that each book reaches a wide and engaged audience, virtually guaranteeing its success.
But that’s not all – NYSORA is equally invested in the digital sphere. All our books are available digitally through our dedicated apps on the Apple Store and Google Play, brought to life by our expert in-house IT, and digital marketing teams: https://lnkd.in/eMzx2t2G
So, if you’ve ever dreamed of publishing a top-tier book but were hesitant due to concerns about support or market success, it’s time to connect with us at NYSORA Press. We’re ready to help turn your dream into reality. Imré Van Herreweghe Ana M López Gutiérrez D. John Doyle Sadiq Bhayani Magnus Wennerlund Kenneth Candido Ivan Keser
#WorldBookDay #NYSORA #MedicalPublishing #Anesthesiology #PainManagement #MSK #POCUS #EmergencyMedicine #DigitalMarketing #MedicalEducation #PublishingSuccess #NYSORAPress #ReadersCommunity #BookLovers

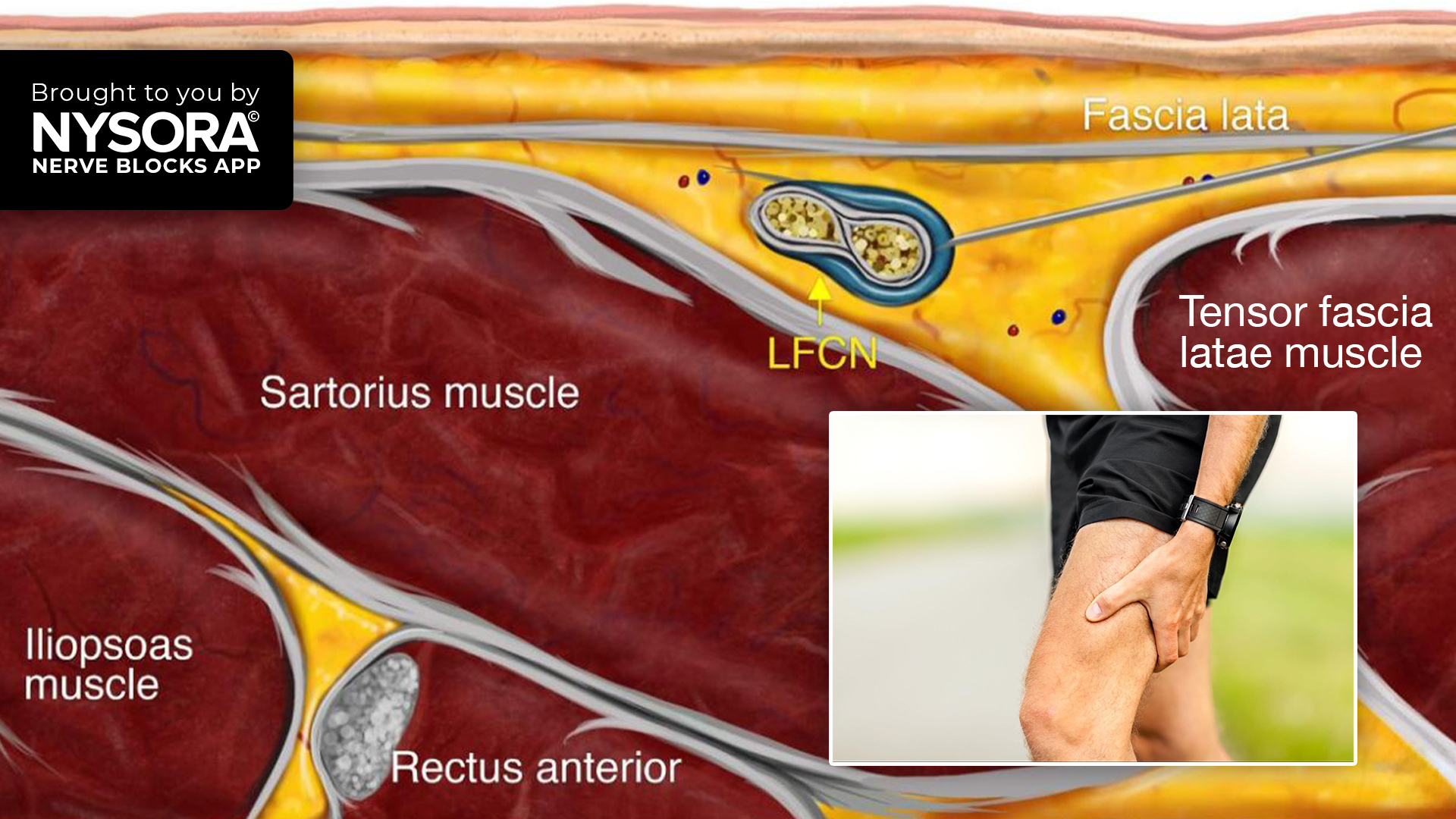
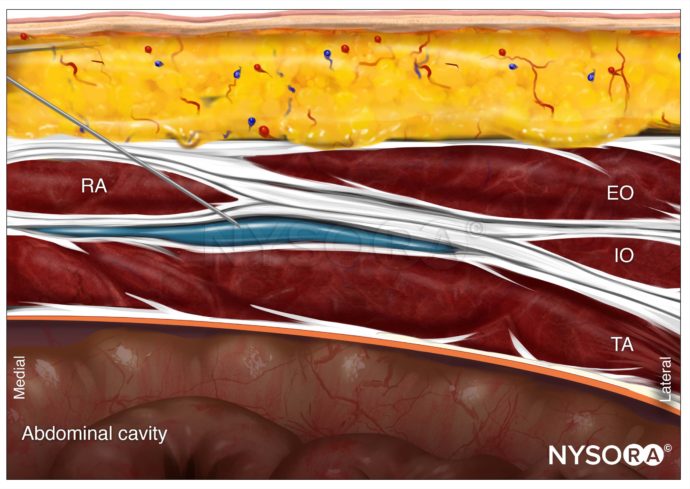
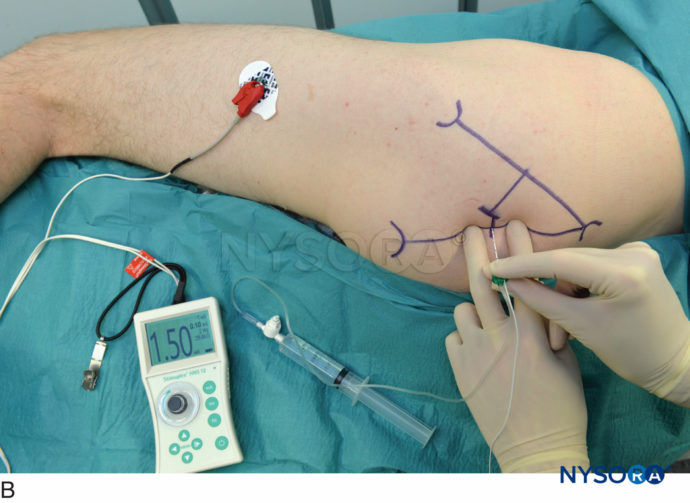
Have you encountered cases of meralgia paresthetica or performed ultrasound-guided nerve blocks like the LFCN block described here? Share your experiences on the effectiveness of such interventions in alleviating pain and improving patient outcomes.
Join our mailing list and get weekly educational updates delivered straight to your inbox.




 Leuven, Belgium
Leuven, Belgium