Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the underlying mechanisms of AR
- Recognize the symptoms of AR
- Manage patients with AR
Definition & mechanisms
- Aortic regurgitation (AR) is defined as diastolic reversal of blood flow from the aorta into the left ventricle
- Most common etiology: Atherosclerotic degeneration of the valve, especially in the presence of a bicuspid aortic valve
- Acute AR:
- May develop from:
- Valvular abnormalities (most commonly infective endocarditis)
- Aortic abnormalities (mostly aortic dissection)
- Iatrogenic causes such as traumatic injury (i.e., motor vehicle accident) or during transcutaneous aortic valve procedures
- Characterized by an abrupt increase in left ventricular end-diastolic volume
- In severe cases, patients often present with pulmonary edema and even cardiogenic shock
- May develop from:
- Chronic AR:
- Most commonly caused by atherosclerotic degeneration of the valve and/or congenital bicuspid aortic valve
- In the early phases, compensatory mechanisms keep the left ventricular ejection fraction in the normal range
- Over time, the LV dilates and hypertrophies to normalize wall stress by maintaining the ratio of ventricular wall thickness to cavity radius
- Compensatory mechanisms allow patients to remain stable and asymptomatic for many years, even in the presence of severe AR
- If wall thickening fails to keep up with the volume overload, there is an increase in wall stress which then results in a reduction in LV systolic function and LVEF due to myocyte damage
- As LV filling pressures rise, symptoms of fatigue and dyspnea may appear
- Angina can develop even in the presence of normal coronary arteries
- Pulmonary edema and heart failure can occur due to chronically elevated left-sided filling pressures
Signs & symptoms
- Symptoms
- Chronic AR
- Patients with chronic AR remain asymptomatic for years. When symptoms appear, they are due to left heart failure:
- Chest pain
- Increasing exercise intolerance
- Dyspnea
- Paroxysmal nocturnal dyspnea
- Orthopnea
- Patients with chronic AR remain asymptomatic for years. When symptoms appear, they are due to left heart failure:
- Acute AR
- Because of a lack of chronic compensation, patients usually present with pulmonary edema and heart failure refractory to optimal medical therapy
- Patients are often hypotensive and clinically appear to be on the verge of cardiovascular collapse
- Chronic AR
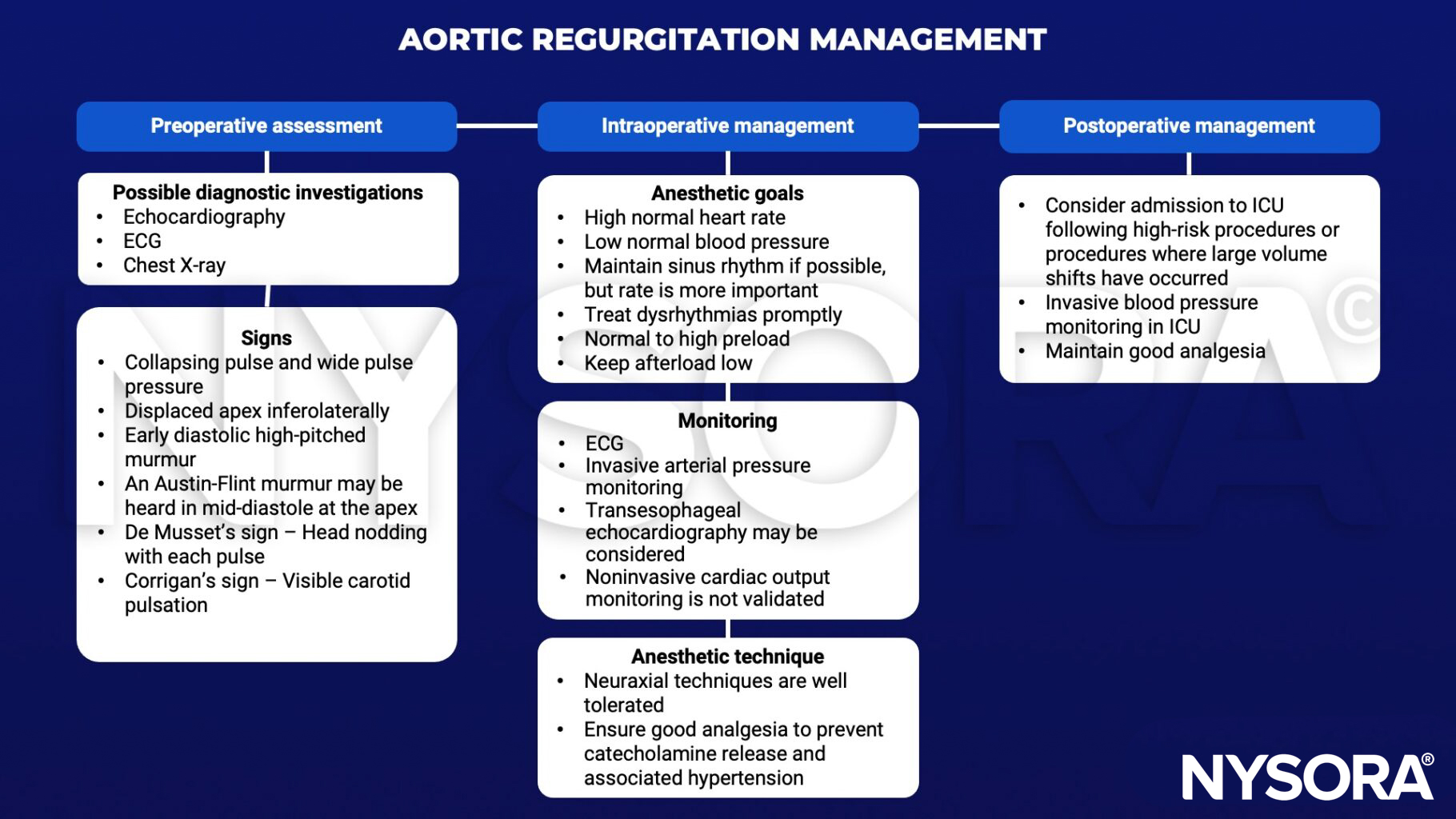
- Diagnostic signs
- Collapsing pulse and wide pulse pressure
- Displaced apex inferolaterally
- Early diastolic high-pitched murmur
- An Austin-Flint murmur may be heard in mid-diastole at the apex
- De Musset’s sign – Head nodding with each pulse
- Corrigan’s sign – Visible carotid pulsation
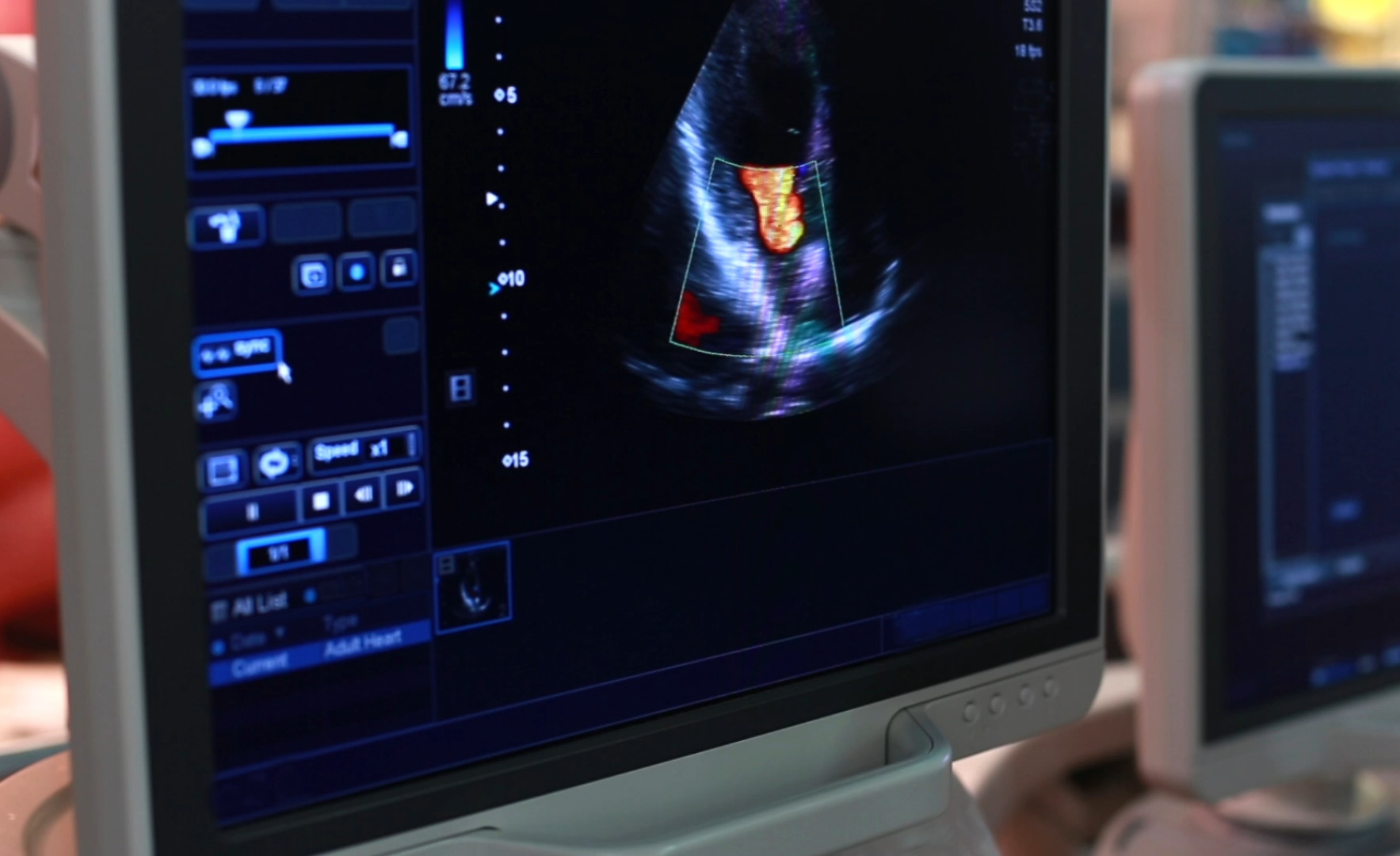
Severity assessment
- Echocardiography is the best diagnostic tool to evaluate the severity of AR. A rough guideline for approximating severity is the width of the AR jet compared to the width of the left ventricular outflow tract:
- <1/3: Mild
- 1/3–2/3: Moderate
- >2/3: Severe
Management
Acute severe AR management
- Sudden aortic incompetence results in acute pulmonary congestion
- Immediate management:
- Afterload reduction (nitroprusside)
- Enhancement of contractility and heart rate (dobutamine)
- Emergency surgical intervention is likely necessary
- Intra-aortic balloon pump is contraindicated
Suggested reading
- Flint N, Wunderlich NC, Shmueli H, Ben-Zekry S, Siegel RJ, Beigel R. Aortic Regurgitation. Curr Cardiol Rep. 2019;21(7):65.
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Hines, R. L. (2017). Stoelting’s anesthesia and co-existing disease (7th ed.). Elsevier – Health Sciences Division
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [published correction appears in Circulation. 2014 Jun 10;129(23):e650]. Circulation. 2014;129(23):2440-2492.