Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Diagnose an inhaled foreign body
- Manage patients with an inhaled foreign body
Background
- Inhaled foreign bodies are a common emergency in young children
- Due to the high position of the larynx and epiglottis and narrow airways, there is a high risk of foreign body aspiration in this age group
- Loss of concentration during physical activity, while eating, or when exploring plastic or metallic objects by putting them in their mouth can result in sudden symptoms of breathing difficulties
- Fourth leading cause of death in young children
- More often in boys compared to girls
Signs & diagnosis
- Signs depend on the type of foreign body, time after aspiration, and exact location of the object, and can range from asymptomatic to severe respiratory distress
- Patients usually present with coughing, wheezing, dyspnea, and rarely with stridor, choking signs, and cyanosis
- The more proximal, the more severe the symptoms
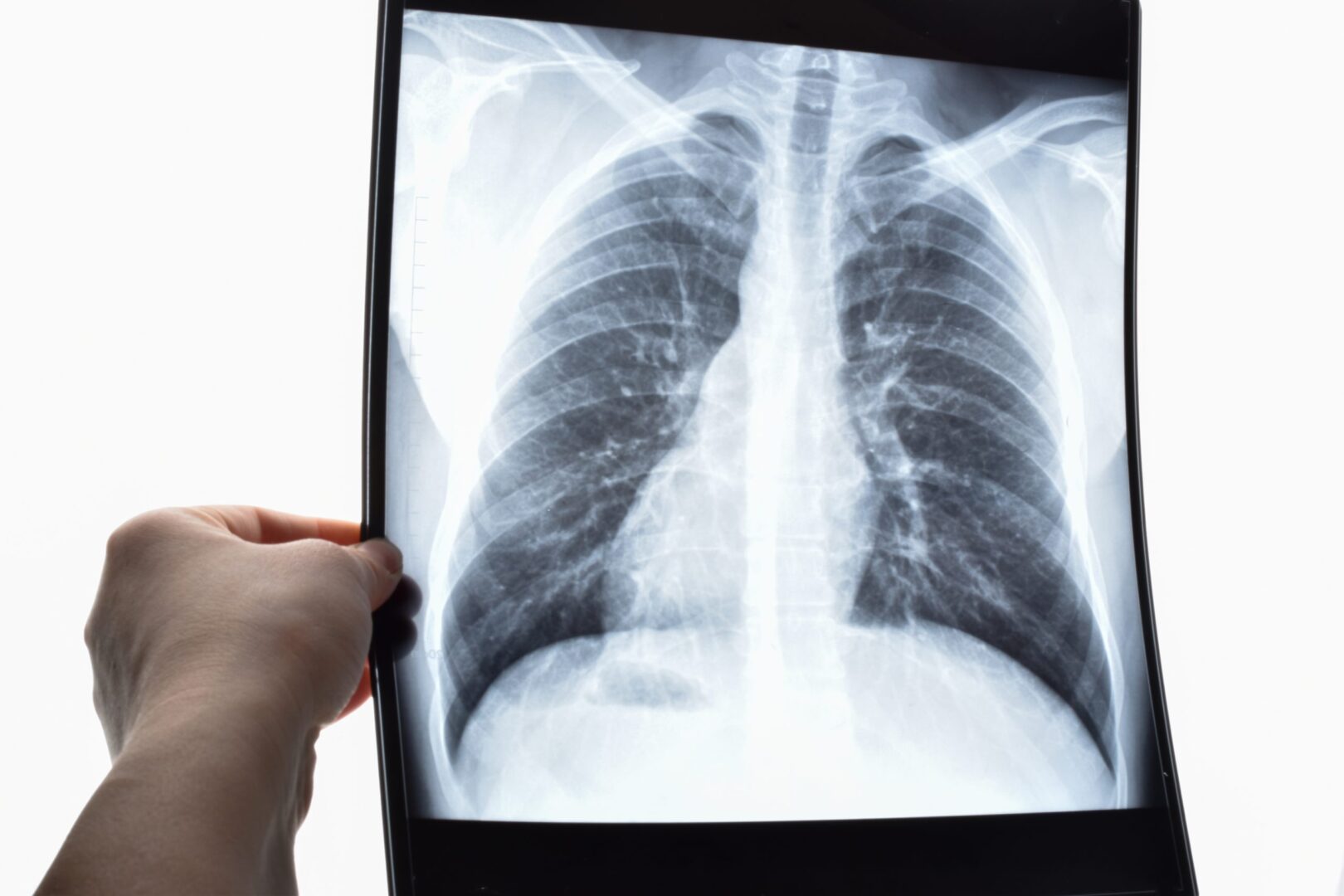
- Many aspirated objects are not radiopaque, resulting in normal-appearing chest radiographs
- Pulmonary infectious or inflammatory infiltration, mediastinal shift, obstructive emphysema, atelectasis, air trapping, and very rarely pneumothorax or pneumomediastinum may be observed
- Normal X-ray results are usually associated with upper airway obstruction, emphysema and infiltration are seen more in distal airway obstruction
- Some organic materials may swell due to fluid absorption, resulting in increased airway blockage
- Sharp objects may perforate the airways
- Eliminate other diagnoses
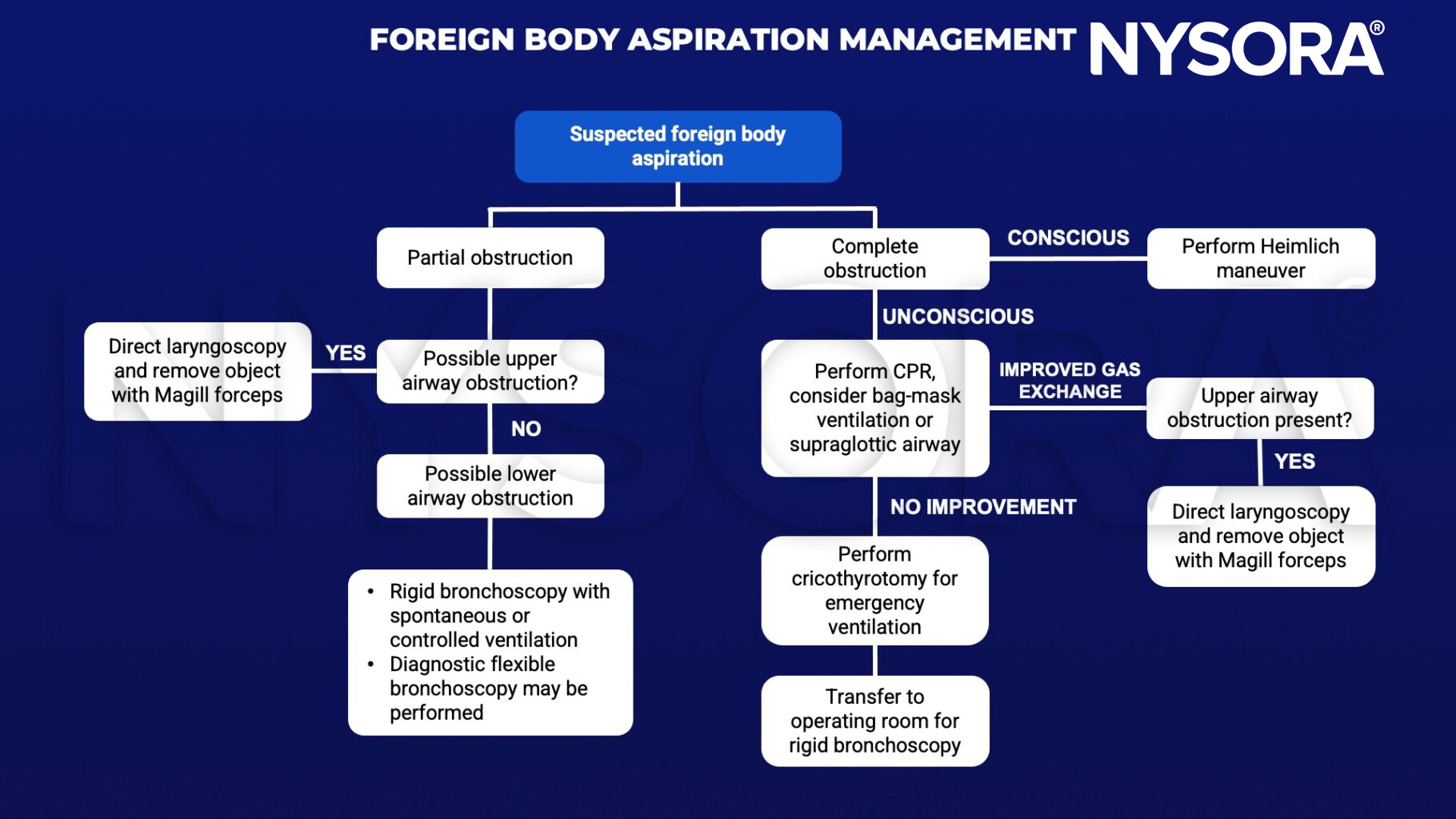
Management
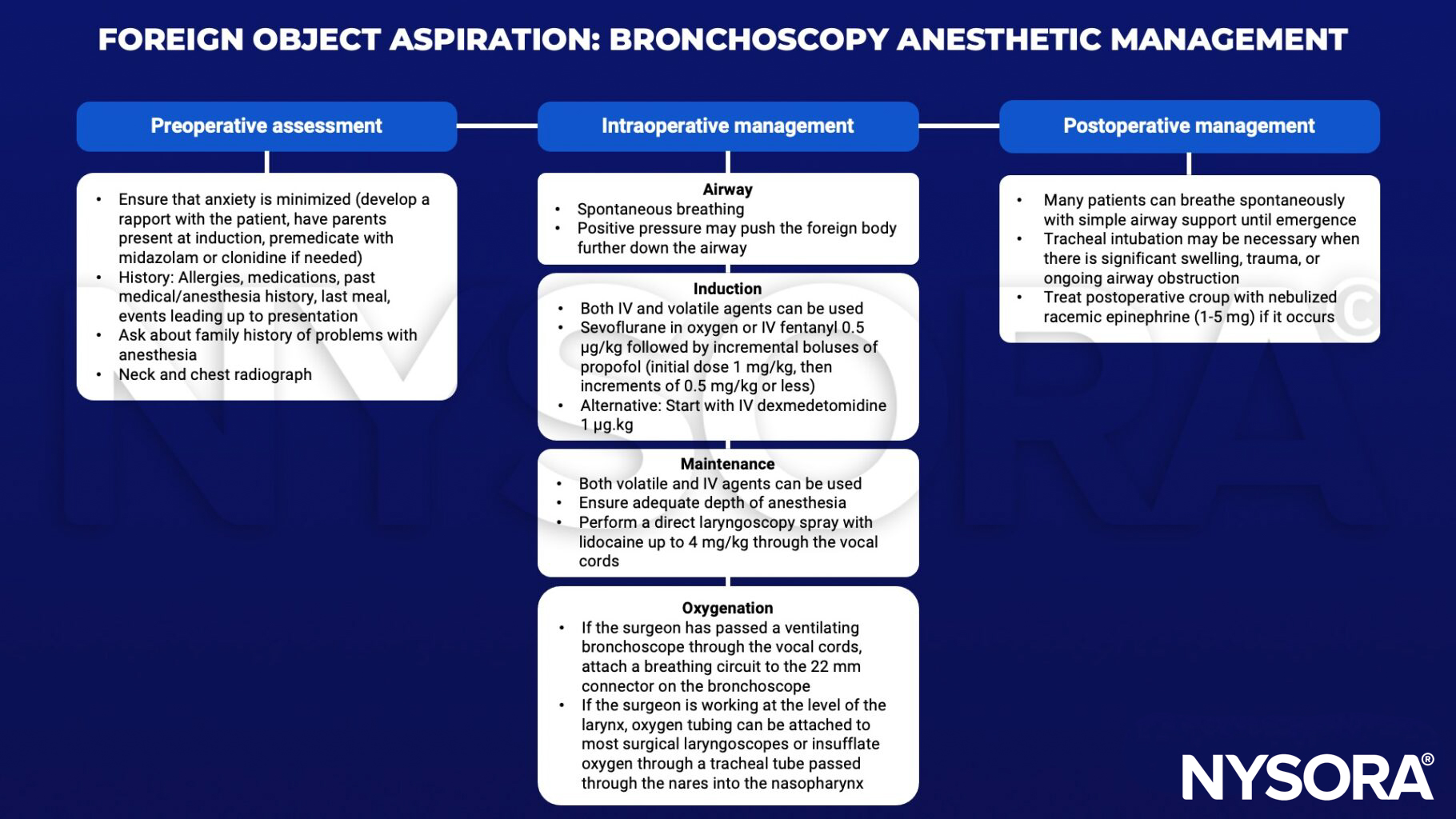
Rigid bronchoscopy anesthetic management
Suggested reading
- Rose D, Dubensky L. Airway Foreign Bodies. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539756/
- Bould MD. Essential notes: the anaesthetic management of an inhaled foreign body in a child. BJA Education. 2019;19(3):66-7.
- Kendigelen P. The anaesthetic consideration of tracheobronchial foreign body aspiration in children. J Thorac Dis. 2016;8(12):3803-3807.
- Moehrle NP, Jagannathan N. Management of foreign body aspiration in pediatric and adult patients. In: Berkow LC, Sakles JC, eds. Cases in Emergency Airway Management. Cambridge: Cambridge University Press; 2015:79-88.