Learning objectives
- Recognize airway trauma
- Management of airway trauma
Definition and mechanism
- A life-threatening condition resulting from blunt and penetrating injuries to the neck and chest, as well as from medical procedures that may injure the airway
- Maxillofacial, neck, or laryngeal trauma
- Airway obstruction or obstruction by blood, secretions, tissue edema, debris, and vomitus
- Airway trauma can be associated with cervical spine injury which will worsen during intubation
Signs and symptoms
- Neck pain
- Hoarseness
- Dysphagia
- Cough
- Dysphonia
- Laryngeal dyspnea
- Loss of consciousness
- Stridor
- Cyanosis
- Hypoxemia
- Hamman’s sign or a mediastinal crunch (a crunching, rasping sound, heard over the precordium in mediastinal emphysema)
Blunt airway injury
| Anatomical territory | Associated problems | Caution: red flag signs and symptoms |
|---|---|---|
| Maxillofacial | Traumatic brain injury and base of skull fracture Cervical spine fracture Ophthalmic injury Vascular injury Pulmonary aspiration of blood and debris | Signs of Increased intracranial pressure Neurological deficit Neurogenic shock Significant bleeding from fracture displacement Bilateral anterior mandible fractures and airway obstruction Ventilatory failure |
| Laryngotracheal | Cervical fracture Vascular injury Oesophageal injury Rib fractures and flail segment Pneumothorax Haemothorax Pneumomediastinum Pulmonary contusion | Massive hemoptysis and stridor have previously been reported as cardinal features of severe laryngotracheal trauma Massive surgical emphysema Ventilatory failure Cardiovascular collapse |
| Trachea and bronchi | Vascular injury Oesophageal injury Rib fractures and flail segment Tension pneumothorax Hemothorax Pneumomediastinum Pulmonary contusion | Massive hemoptysis Massive surgical emphysema Ventilatory failure Cardiovascular collapse |
Management
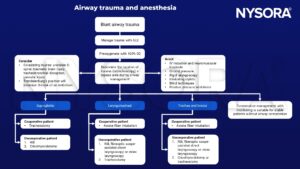
Keep in mind
- Full stomach vs difficult airway vs need for double-lumen tube
- Airway management may be difficult in the uncooperative or pediatric patient
Suggested reading
- Shilston J, Evans DL, Simons A, Evans DA. Initial management of blunt and penetrating neck trauma. BJA Educ. 2021;21(9):329-335.
- Mercer SJ, Jones CP, Bridge M, Clitheroe E, Morton B, Groom P. Systematic review of the anaesthetic management of non-iatrogenic acute adult airway trauma. Br J Anaesth. 2016;117 Suppl 1:i49-i59.
- Jain U, McCunn M, Smith CE, Pittet JF. Management of the Traumatized Airway. Anesthesiology. 2016;124(1):199-206.
- Prokakis C, Koletsis EN, Dedeilias P, Fligou F, Filos K, Dougenis D. Airway trauma: a review on epidemiology, mechanisms of injury, diagnosis and treatment. J Cardiothorac Surg. 2014;9:117.
We would love to hear from you. If you should detect any errors, email us at customerservice@nysora.com