
Learning objectives
- Diagnose and treat calcium blocker toxicity
Definition and mechanisms
- Calcium channel blockers (CCBs) are used to treat hypertension, supraventricular tachycardia, vasospasm, and migraine headaches
- Ingestion of excessive CCB agents is one of the most potentially lethal prescription drug overdoses
- Overdoses of immediate-release CCBs are characterized by rapid progression to hypotension, bradydysrhythmia, and cardiac arrest
- Overdoses of extended-release formulations result in delayed onset of dysrhythmias, shock, sudden cardiac collapse, and bowel ischemia
- Symptoms occur within six hours after ingestion, although some forms of medication do not start until after 24 hours
- Calcium channel blockers target the L-type voltage-gated calcium channels and these are predominant in the following sites and roles:
- Depolarization of the sinoatrial node (SA) and impulse propagation through the atrioventricular node (AV).
- Three main classes of CCBs:
- Phenylalkylamines (verapamil)
- Benzothiazepines (diltiazem)
- Dihydropyridines (nifedipine, amlodipine, felodipine, isradipine, nicardipine, nimodipine)
Signs and symptoms
- Dizziness
- Fatigue
- Nausea and vomiting
- Lightheadedness
- Altered mental status
- Coma
- Dyspnea
- Hypotension
- Bradycardia
- Hyperglycemia
- Metabolic acidosis
- Hypokalemia
- Hypocalcemia
- Pulmonary edema
- Renal failure
Diagnosis
- Hyperglycemia
- Blood gas: hyperlactatemia, metabolic acidosis, impaired oxygen delivery
- ECG:
- Bradycardia
- QT prolongation
- Bundle branch block
- First-degree atrioventricular block
- Junctional rhythms
- Sinus tachycardia (dihydropyridines)
- Echocardiography
- Chest X-ray: pulmonary edema
Complications
| Complications from toxicity | Complications from treatment |
|---|---|
| Refractory cardiogenic and distributive shock | Multiorgan failure from calciphylaxis with overaggressive calcium infusion |
| Acute Respiratory Distress Syndrome | Hypokalemia and Hypoglycemia |
| Severe hypoperfusion and resultant end-organ injury like ischemic bowel, myocardial infarction, acute tubular necrosis, limb necrosis | Acute Respiratory Distress Syndrome hypertriglyceridemia, pancreatitis, and fat overload syndrome with lipid emulsion therapy |
| Pulseless electrical activity with cardiac arrest (PEA) | Nausea, vomiting, ileus, and Hypokalemia with glucagon |
| Arterial and venous thrombosis and limb ischemia with interventions like ECMO |
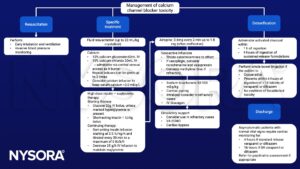
Management
Suggested reading
- Alshaya, O.A., Alhamed, A., Althewaibi, S., Fetyani, L., Alshehri, S., Alnashmi, F., Alharbi, S., Alrashed, M., Alqifari, S.F., Alshaya, A.I., 2022. Calcium Channel Blocker Toxicity: A Practical Approach. Journal of Multidisciplinary Healthcare Volume 15, 1851–1862.
- Jackson, R., Bellamy, M., 2015. Antihypertensive drugs. BJA Education 15, 280–285.
- St-Onge M, Dubé PA, Gosselin S, et al. Treatment for calcium channel blocker poisoning: a systematic review. Clin Toxicol (Phila). 2014;52(9):926-944.
- Kerns W 2nd. Management of beta-adrenergic blocker and calcium channel antagonist toxicity. Emerg Med Clin North Am. 2007;25(2):309-viii.
We would love to hear from you. If you should detect any errors, email us customerservice@nysora.com







