Learning objectives
- Describe hyperaldosteronism
- Recognize the symptoms and signs of hyperaldosteronism
- Anesthetic management of a patient with hyperaldosteronism
Definition and mechanisms
- Hyperaldosteronism is a condition in which one or both adrenal glands produce too much aldosterone
- Aldosterone regulates blood pressure by controlling blood levels of potassium and sodium
Classification
- Primary hyperaldosteronism (Conn’s syndrome): Overproduction of aldosterone independent from the renin-angiotensin-aldosterone system (RAAS), usually caused by a tumor of the adrenal gland
- Secondary hyperaldosteronism (hyperreninism): Overproduction of aldosterone due to overactivity of the RAAS
Signs and symptoms
- Hypertension
- Headache
- Dizziness
- Vision changes
- Difficulty breathing
- Fluid and electrolyte imbalances
- Hypokalemia
- Muscle weakness
- Muscle spasm
- Tingling and numbness
- Fatigue
- Polydipsia
- Polyuria
- Hypernatremia
- Hypermagnesemia
- Metabolic alkalosis
- Volume depletion
- Hypokalemia
Complications
The most common complications are caused by hypertension
- Atrial fibrillation
- Left ventricular hypertrophy
- Heart attack
- Stroke
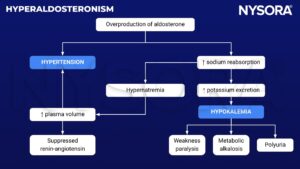
Pathophysiology
Treatment
Primary hyperaldosteronism
- Surgery to remove the adrenal gland tumor
- Potassium-sparing diuretics that act as aldosterone antagonists (i.e., spironolactone, eplerenone, and amiloride)
- Limit salt intake
Secondary hyperaldosteronism
- No surgery
- Potassium-sparing diuretics that act as aldosterone antagonists (i.e., spironolactone, eplerenone, and amiloride)
- COX-2 inhibitors
- Limit salt intake
Management
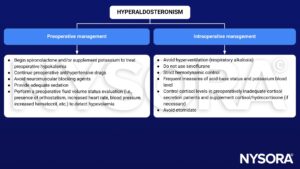
Keep in mind
- The anesthesiologist must deal with hypertension, hypovolemia, hypokalemia, and cortisol supplementation (depending case by case) in patients with hyperaldosteronism
Suggested reading
- Domi R, Sula H, Kaci M, Paparisto S, Bodeci A, Xhemali A. Anesthetic considerations on adrenal gland surgery. J Clin Med Res. 2015;7(1):1-7.
- Jano A, Domi R, Berdica L, et al. Anaesthetic considerations of Conn syndrome: a case presentation and mini-review the anaesthesiologist and Conn syndrome. Clin Med Res 2014;3(5):132–135.
- Davies M, Hardman J. Anaesthesia and adrenocortical disease. Continuing Education in Anaesthesia, Critical Care & Pain. 2005;5(4):122–126.
We would love to hear from you. If you should detect any errors, email us customerservice@nysora.com