
Learning objectives
- Recognize the signs of POD
- Identify risk factors for POD
- Reduce the risk of POD in susceptible patients
- Manage POD occurrence
Definition
- Postoperative delirium (POD) is defined as an acute onset fluctuating change in mental status characterized by reduced awareness of the environment and disturbance of attention
- It is a temporary neurocognitive syndrome observed after surgery
- Incidence in older surgical patients varies from 7% to 53%
- POD prolongs postoperative ventilation, intensive care, length of stay, increases costs, and negatively impacts functional outcome and survival
Signs
3 subtypes:
- Hyperactive: Restlessness, agitation, and hypervigilance, often hallucinations and delusions
- Hypoactive: Lethargy and sedation, slow response to questioning, little spontaneous movement
- Mixed: Both hyperactive and hypoactive features
Risk factors
| Predisposing | Precipitating |
|---|---|
| Advanced age | ICU admission |
| Male sex | High-risk surgical procedure |
| Low body mass index | Sleep deprivation |
| Sight/hearing loss | Polypharmacy |
| Social isolation | Medications |
| Multimorbidity | Severe illness (e.g. infection, fracture, stroke) |
| Prior cognitive impairment | Hyper- or hypothermia |
| Malnutrition | Sensory deprivation |
| Low serum albumin | Increasing duration of surgery |
| Frailty | Urgency of surgery |
| Cancer | Pain |
| Alcohol/drug abuse | Perioperative complications |
| Antipsychotics | Hypoxia |
| Malnutrition | Physical restraints |
| Dehydration | Prolonged use of catheters |
| Depression | |
Prevention
- Identify risk factors
- Frailty assessment
- Bispectral index (BIS) monitoring (Target BIS 40-60)
- Avoid benzodiazepines
- Multi-component interventions (visual and hearing aids, sleep promotion, minimalization of catheters/cannulae…)
- Regional anesthesia instead of general
- Treat pain (multimodal strategy)
- Prehabilitation programs that improve physical and cognitive capacity
Preventative measures requiring further investigation:
- Total intravenous anesthesia (TIVA)
- Lighter sedation
- Dexmedetomidine
- Melatonin
- Steroids
- Cholinergic stimulation
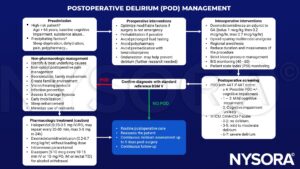
Management
Suggested reading
- Hoogma, Danny Feike; Milisen, Koen; Rex, Steffen; Al tmimi, Layth. Postoperative delirium: identifying the patient at risk and altering the course: A narrative review. European Journal of Anaesthesiology and Intensive Care 2(3):p e0022, June 2023.
- Mossie A, Regasa T, Neme D, Awoke Z, Zemedkun A, Hailu S. Evidence-Based Guideline on Management of Postoperative Delirium in Older People for Low Resource Setting: Systematic Review Article. Int J Gen Med. 2022;15:4053-4065.
- Swarbrick CJ, Partridge JSL. Evidence-based strategies to reduce the incidence of postoperative delirium: a narrative review. Anaesthesia. 2022;77 Suppl 1:92-101.
- Subramaniam B, Shankar P, Shaefi S, et al. Effect of Intravenous Acetaminophen vs Placebo Combined With Propofol or Dexmedetomidine on Postoperative Delirium Among Older Patients Following Cardiac Surgery: The DEXACET Randomized Clinical Trial [published correction appears in JAMA. 2019 Jul 16;322(3):276]. JAMA. 2019;321(7):686-696.
- Haque N, Naqvi RM, Dasgupta M. Efficacy of Ondansetron in the Prevention or Treatment of Post-operative Delirium-a Systematic Review. Can Geriatr J. 2019;22(1):1-6. Published 2019 Mar 30.
- Khan BA, Perkins AJ, Gao S, et al. The Confusion Assessment Method for the ICU-7 Delirium Severity Scale: A Novel Delirium Severity Instrument for Use in the ICU. Crit Care Med. 2017;45(5):851-857.
- Chan MT, Cheng BC, Lee TM, Gin T; CODA Trial Group. BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J Neurosurg Anesthesiol. 2013;25(1):33-42.
- Fong TG, Tulebaev SR, Inouye SK. Delirium in elderly adults: diagnosis, prevention and treatment. Nat Rev Neurol. 2009;5(4):210-220.
- Robinson TN, Eiseman B. Postoperative delirium in the elderly: diagnosis and management. Clin Interv Aging. 2008;3(2):351-355.
We would love to hear from you. If you should detect any errors, email us at customerservice@nysora.com












