
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the wide variety of signs and symptoms of serotonin syndrome (SS)
- Management of a patient with SS
Definition and mechanisms
- The serotonin syndrome (SS) is a potentially life-threatening drug interaction caused by excessive serotoninergic activity in the CNS
- Can arise from therapeutic drug use, drug interactions, or intentional overdose of medications that affect the serotonergic system, use the mnemonic MAD HOT:
- Myoclonus
- Autonomic instability
- Delirium, Diarrhea
- Hot (fever)
- CNS: seizure, altered LOC
- CVS: tachycardia & HTN, autonomic instability, arrhythmia
- MSK: rigidity, rhabdomyolysis, hyperkalemia & renal failure
- Hyperthermia
- Disseminated intravascular coagulation
- Onset of SS typically occurs all of a sudden within 24-48h of exposure to the triggering agents and usually resolves quickly after the triggering agent is discontinued
- Note that the washout period after discontinuation is highly variable between psychotropic drugs
Signs and symptoms
| Mild | Sweating Fever Agitation Confusion Anxiety Tachycardia Diarrhea Tremors Poor coordination |
| Full-blown | Hyperthermia Shivering Diaphoresis Hypomania Hypervigilance Hypertension Hyperreflexia Clonus Myoclonus |
| Severe | Hyperthermia > 40°C Seizures Coma Rigidity |
Differential diagnosis
| Disease | Medication exposure | Shared clinical features | Distinguishing clinical features |
|---|---|---|---|
| Serotonin Syndrome | Serotonergic medications | Hypertension | Clonus Hyperreflexia Hyperactive bowel sounds |
| Neuroleptic malignant syndrome | Dopamine antagonists | Tachycardia | No clonus or hyperreflexia Bradykinesia |
| Anticholinergic toxicity | Acetylcholine antagonist | Hyperthermia | No clonus or hyperreflexia Dry skin Absent bowel sounds |
| Malignant hyperthermia | Halogenated anesthetics Succinylcholine | Altered mental status | No clonus or hyperreflexia Extreme muscular rigidity |
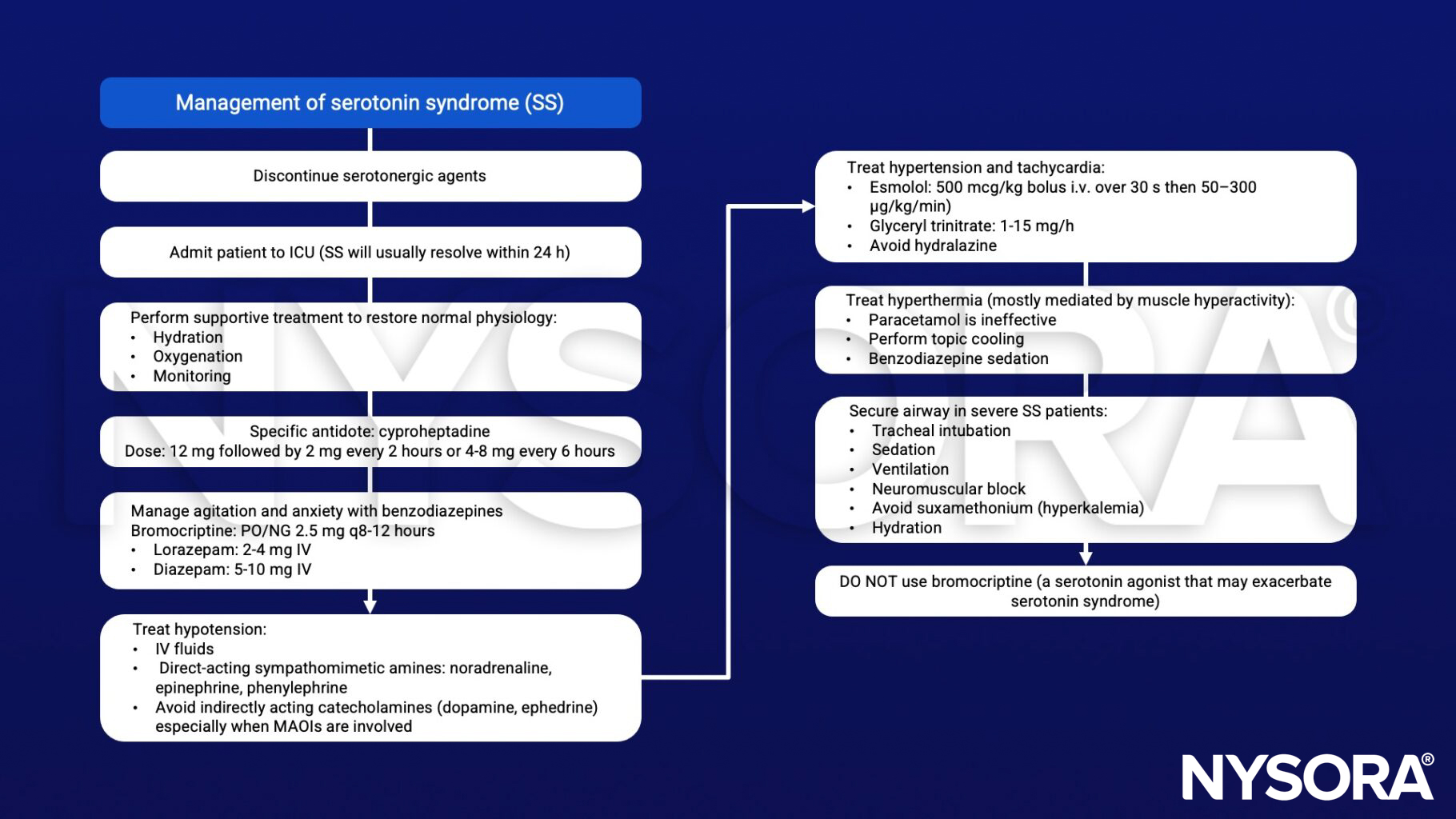
Management
Suggested reading
- Bartakke, A., Corredor, C., Van Rensburg, A., 2020. Serotonin syndrome in the perioperative period. BJA Education 20, 10–17.
- Francescangeli, J., Karamchandani, K., Powell, M., Bonavia, A., 2019. The Serotonin Syndrome: From Molecular Mechanisms to Clinical Practice. International Journal of Molecular Sciences 20, 2288.
- Chinniah, S., French, J.L.H., Levy, D.M., 2008. Serotonin and anaesthesia. Continuing Education in Anaesthesia Critical Care & Pain 8, 43–45.
Clinical updates
Bai et al. (JAMA Network Open, 2022) conducted a population-based cohort study of 1134 older outpatients prescribed oral linezolid and found serotonin syndrome occurred in fewer than 0.5% of patients, with no significant increase in risk among the 19% taking concomitant antidepressants. In propensity score–matched analysis, the adjusted risk difference was −1.2%, indicating that even in the worst-case scenario, antidepressants would increase the risk by at most 0.5%, with no differences in hospitalization, altered mental status, or mortality, supporting that linezolid can generally be used safely with antidepressants while maintaining vigilance.
Spadaro et al. (The Journal of Emergency Medicine, 2022) provide an ED-focused review emphasizing that serotonin syndrome is a high-morbidity toxidrome characterized by neuromuscular hyperactivity (clonus in 60–79%, hyperreflexia), autonomic instability, and altered mental status, with mortality primarily related to severe hyperthermia >41°C . They highlight the Hunter Criteria as most applicable in the ED (84% sensitivity, 97% specificity), identify common implicated agents from the ToxIC registry (sertraline, dextromethorphan, citalopram, bupropion, fluoxetine), and stress that management centers on benzodiazepine sedation, rapid external cooling (ice immersion for severe hyperthermia), avoidance of succinylcholine and fentanyl, and limited utility of cyproheptadine in critically ill patients.











