Learning objectives
- Understand the indications and contraindications for tonsillectomy
- Anesthetic management for patients undergoing tonsillectomy
- Discuss the management of post-tonsillectomy bleeding
Definition and mechanisms
- Tonsillectomy is a surgical procedure to remove the palatine tonsils, which are lymphoid tissue covered in the respiratory epithelium and invaginated to create crypts
- It is a common procedure in children to treat recurrent acute sore throat
- Adenotonsillar hypertrophy can present with nasal obstruction, recurrent infections, secretory otitis media, deafness (secondary to Eustachian tube dysfunction), and obstructive sleep apnea (OSA)
- The surgery is performed through the mouth using a Boyle-Davis gag → difficulties may be encountered due to a poorly placed gag, obstructing the tracheal tube or laryngeal mask airway
Patient characteristics
- Chronic/recurrent throat infections
- Comorbidities
- OSA
- Congenital abnormalities (e.g., Down syndrome)
- May have malignancy
- Other incidental medical conditions
- Cor pulmonale due to long-term hypoxia
Indications and contraindications for surgery
Absolute indications
- Upper airway obstruction, dysphagia, and OSA
- Peritonsillar abscess, which is unresponsive to adequate medical management and surgical drainage
- Recurrent tonsillitis with associated febrile convulsions
- Requirement for biopsy to confirm tissue pathology
Relative indications
- Recurrent tonsillitis, which is unresponsive to medical treatment
- Sore throat secondary to tonsilitis
- >5 episodes of tonsillitis in one year
- Symptoms >1 year
- Episodes of sore throats are disabling
- Persistent bad breath and taste in the mouth due to chronic tonsillitis
- Persistent tonsillitis in streptococcus carrier, which is unresponsive to beta-lactamase-resistant antibiotics
- Pathology thought to be neoplastic
Contraindications
- Bleeding diathesis
- Acute infection
- Anemia
- Significant anesthetic risk
Management
Post-tonsillectomy bleeding
- Serious complication of tonsillectomy that can occur in the recovery or hours later
- Emergency with limited time to optimize
- Persistent swallowing can be an early indicator of bleeding from the tonsillar bed
- Patient may be hypovolemic and require fluid resuscitation before induction → assess patient’s fluid status and cardiovascular parameters
- Risk of aspiration due to potential full stomach with blood
- Potential difficult airway due to blood in the airway and edema from recent intubation
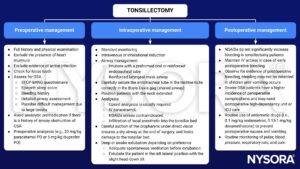
Intraoperative management
- Resuscitate patients and apply full monitoring
- Assess previous anesthetic record
- Suction must be immediately available
- Head-down tilt helps to drain blood away from the larynx
- Rapid sequence induction ensures quick intubation and protects the airway during induction
- Intubation may require a smaller sized endotracheal tube than originally inserted
- Continue fluid resuscitation throughout surgery
- Empty the stomach with a wide-bore naso- or orogastric tube, and ensure that the stomach is empty before extubation
- Extubate patients only when fully awake, in the head-down, left lateral position
Postoperative management
- Patients have to stay in the recovery for an extended period to ensure that the bleeding has stopped
- Check the hemoglobin and coagulation, and transfuse blood if necessary
- Closely monitor patients for further bleeding
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 19 ENT Surgery, MacNab R, Bexon K, Clegg S, Hutchinson A.
- Davies K. Anaesthesia for tonsillectomy. WFSA. April 2, 2007. Accessed February 10, 2023. https://resources.wfsahq.org/atotw/anaesthesia-for-tonsillectomy/.
We would love to hear from you. If you should detect any errors, email us customerservice@nysora.com