Learning objectives
- Describe tracheoesophageal fistula and esophageal atresia, and their classification
- Define the associated congenital anomalies of tracheoesophageal fistulas
- Anesthetic management of pediatric patients with a tracheoesophageal fistula and/or esophageal atresia
Definition and mechanisms
- A tracheoesophageal fistula (TEF) is one of the most common congenital anomalies and is an abnormal connection (fistula) between the esophagus and trachea
- TEF commonly occurs with esophageal atresia (EA), a related congenital malformation with a similar presentation to TEF
- EA is an abnormal connection between the esophagus and stomach, the esophagus ends in a blind-ended pouch rather than connecting normally to the stomach, can occur with or without the presence of a fistula
Classification
| Type A | No TEF, only EA → isolated EA The esophagus is divided into two parts with both portions ending in blind pouches | 8% of all cases |
| Type B | Proximal TEF and distal EA The lower portion of the esophagus ends in a blind pouch and the upper portion is connected to the trachea by a TEF | 2% of all cases |
| Type C | Proximal EA and distal TEF The upper portion of the esophagus ends in a blind pouch and the lower portion is connected to the trachea by a TEF | Most common, 85% of all cases |
| Type D | Both proximal and distal TEF TEF connects both the upper and lower portions of the esophagus and trachea | Rarest form, <1% of all cases |
| Type E (H-type) | Isolated TEF The esophagus connects to the stomach normally and is fully intact, a TEF connects the esophagus and trachea | 4% of all cases |
Signs and symptoms
- Excessive oral secretions, salvation
- Breathing difficulties, respiratory distress
- Coughing or choking when feeding
- Vomiting
- Cyanosis, especially during feeding
- Feeding difficulties
- Frequent lung infections
- Risk of aspiration
- EA and the inability to swallow may cause polyhydramnios in utero
Associated congenital anomalies
50% of babies with TEF/EA also have associated congenital anomalies
- Prematurity (30%)
- Congenital heart disease (30%): Ventricular septal defect, tetralogy of Fallot, patent ductus arteriosus, atrial septal defect, right-sided aortic arch
- Gastrointestinal anomalies (14%): Diaphragmatic hernia, duodenal atresia, pyloric stenosis, imperforate anus, malrotation, omphalocele
- Genitourinary anomalies (14%): Renal agenesis, hypospadias, horseshoe/polycystic kidney, ureteric/urethral abnormalities
- Musculoskeletal anomalies (10%): Radial limb abnormalities, polydactyly, lower limb defects, hemivertebrae, rib defects, scoliosis
- VACTERL syndromes (10%)
- Respiratory anomalies (6%): Tracheobronchomalacia, pulmonary hypoplasia, tracheal agenesis/stenosis, tracheal upper pouch
- Chromosome abnormalities (4%): Trisomy 13, 18, or Down syndrome
Treatment
- Surgical correction with resection of any fistula and anastomosis of any discontinuous segments
- Usually repaired within 24 hours of birth to minimize the risk and complications of aspiration
- Complications after surgery
- Anastomotic leaks
- Esophageal strictures (abnormal tightening)
- Damage to the laryngeal nerve
- Recurrence of the fistula
- Gastroesophageal reflux disease
- Dysphagia
- Asthma-like symptoms: Persistent coughing or wheezing
- Recurrent chest infections
- Tracheomalacia
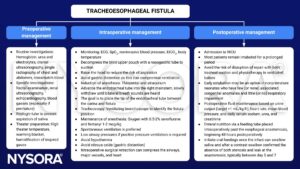
Management
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 24 Paediatrics, Lomas B.
- Choumanovai I, Sanusii A, Evansii F. Anaesthetic management of tracheo-oesophageal fistula/ oesophageal atresia. WFSA. October 17, 2017. Accessed February 16, 2023. https://resources.wfsahq.org/atotw/anaesthetic-management-of-tracheo-oesophageal-fistula-oesophageal-atresia/
- Saraiya NR. TRACHEOESOPHAGEAL FISTULA. In: Houck PJ, Haché M, Sun LS. eds. Handbook of Pediatric Anesthesia. McGraw Hill; 2015. Accessed February 16, 2023. https://accessanesthesiology.mhmedical.com/content.aspx?bookid=1189§ionid=70363324
We would love to hear from you. If you should detect any errors, email us customerservice@nysora.com