Case study: Acromioclavicular joint arthritis – Injection
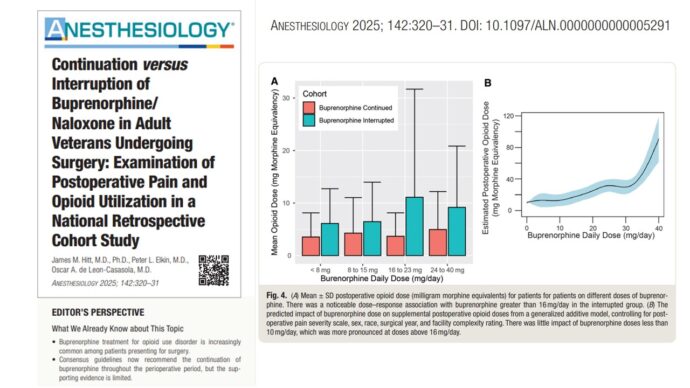
Acromioclavicular (AC) joint arthritis is a common cause of shoulder pain, particularly among individuals who engage in repetitive manual activities. In this article, we will discuss the case of a 65-year-old woman with AC joint arthritis and the use of ultrasound-guided injection as an effective treatment option for pain relief.
Case presentation
A 65-year-old female manual laborer presented with a 4-month history of left shoulder pain. Her symptoms included:
- Pain over the anteromedial region of the shoulder.
- Pain on external rotation.
- Superior shoulder pain, especially at night.
This type of presentation is typical of AC joint arthritis, especially in individuals whose work or lifestyle places frequent stress on their shoulders.
Diagnosis
Physical examination
- Painful arc
- Scarf test: Positive
- O’Brien’s test: Positive
Imaging and laboratory findings
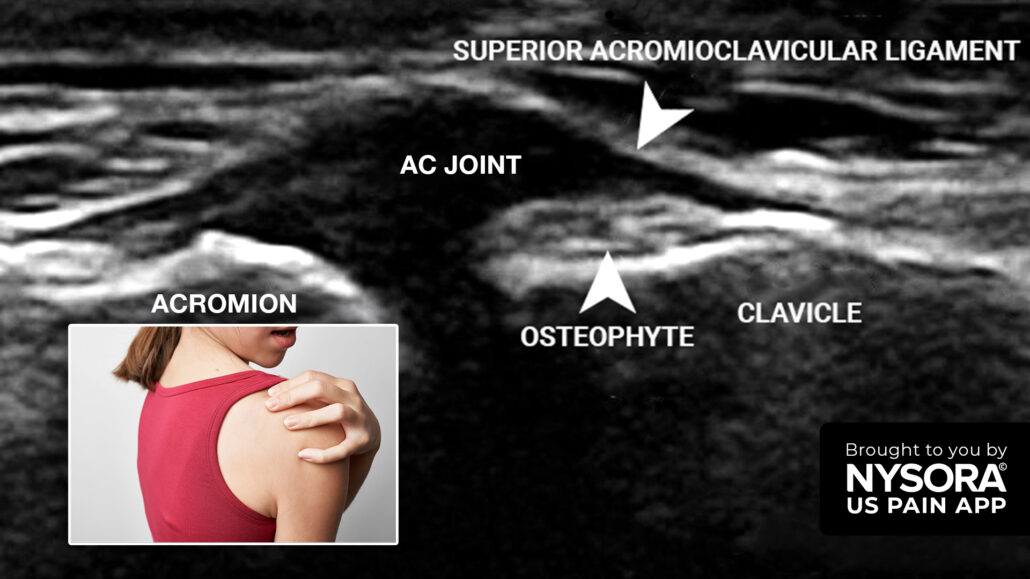
- Ultrasound: An ultrasound of the AC joint showed space narrowing, capsular distension, and the presence of an osteophyte, all consistent with AC joint arthritis.
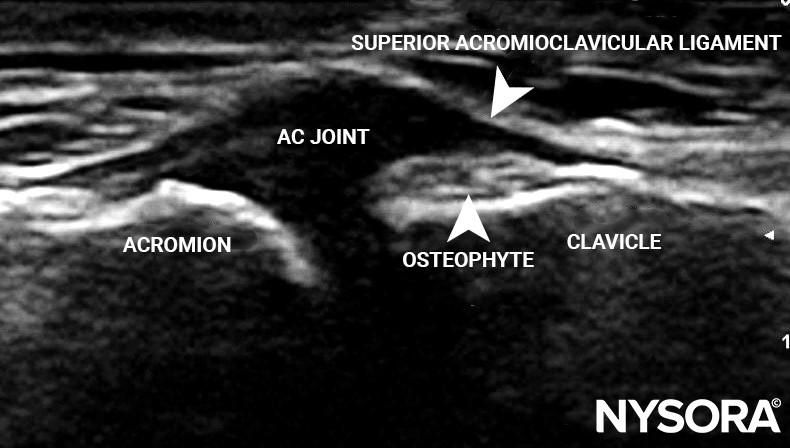
Transverse view of the AC joint space showing space narrowing, capsular distension, and an osteophyte.
- X-ray: X-ray imaging revealed rotator cuff arthropathy and AC joint arthritis, with joint space reduction.
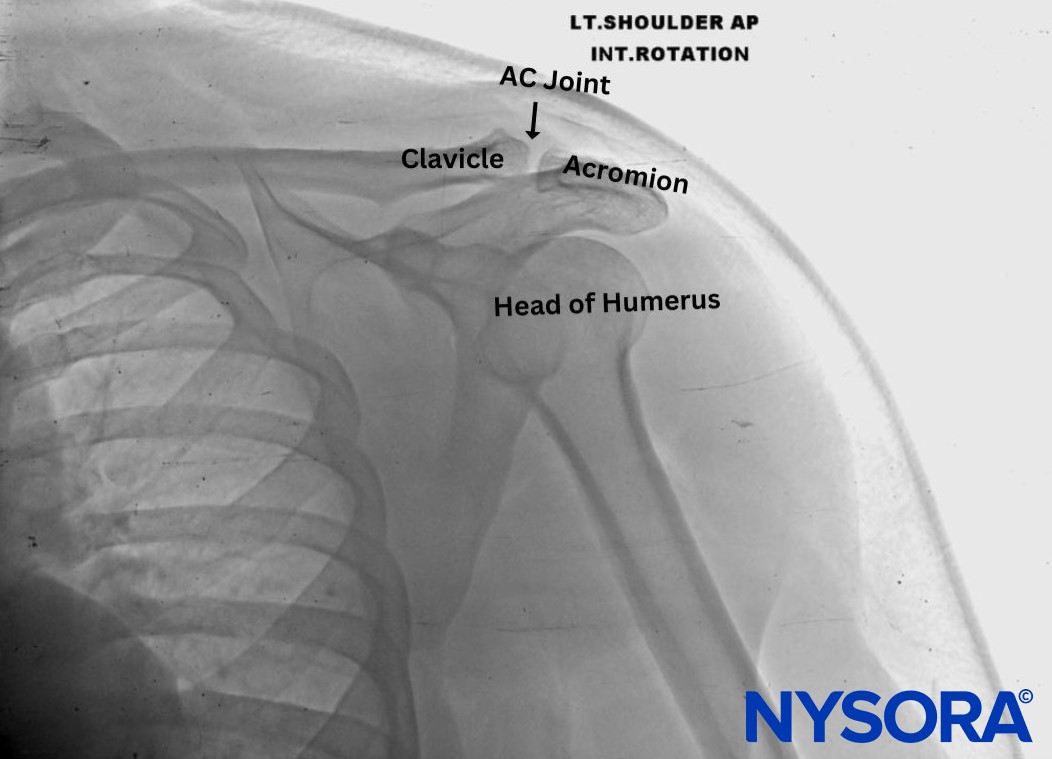
X-ray image of the left shoulder.
- Fasting blood sugar: The patient’s fasting blood sugar was 102 mg/dL, within the normal range, ruling out diabetic complications as a cause of the pain.
Final diagnosis
The patient was diagnosed with acromioclavicular joint arthritis and supraspinatus tendinopathy. AC joint arthritis arises from the deterioration of cartilage within the AC joint, often due to repetitive stress. Supraspinatus tendinopathy is commonly associated with impingement in the subacromial space, leading to inflammation and degeneration of the tendon.
Treatment: Ultrasound-guided AC joint injection
Given the severity of the patient’s pain and the failure of conservative treatment to provide adequate relief, an ultrasound-guided injection of the AC joint was chosen as the next step. This minimally invasive procedure involves the injection of a local anesthetic and corticosteroid to reduce inflammation and alleviate pain.
Technique
Ultrasound Setup
- Transducer Type: 3-13 MHz linear transducer.
- Orientation: Coronal plane, parallel to the floor.
- Depth: 2 cm.
The transducer is positioned on the superior aspect of the shoulder to visualize the AC joint. The acromion and clavicle are identified, along with the superior acromioclavicular ligament. The joint space is examined for signs of arthritis, such as osteophytes and narrowing.
Patient positioning
The patient is positioned supine, with the affected arm positioned to reach toward the ipsilateral knee. This position allows for optimal access to the AC joint.
Needle insertion
The needle is inserted from lateral to medial using an in-plane technique. A 24-gauge, 1.5-inch hypodermic needle is guided under ultrasound visualization to ensure accurate placement under the superior acromioclavicular ligament. The needle is carefully advanced, and a loss of resistance is felt once the ligament is pierced.
- Pharmacological agents:
- 1 mL of 2% lidocaine (local anesthetic)
- 10 mg of triamcinolone (corticosteroid)
This combination provides immediate pain relief from the lidocaine, while the triamcinolone reduces inflammation in the AC joint over the following days to weeks.
Patient outcome
One month after the ultrasound-guided AC joint injection, the patient reported 100% pain relief. She experienced no adverse effects and was able to return to her manual labor job without pain. The long-lasting effects of the corticosteroid allowed her to resume normal activities with minimal discomfort.
Follow-up recommendations
- The patient should follow up with her physician in three to six months to assess the need for additional injections if pain recurs.
- A tailored physical therapy program focusing on shoulder strengthening and range-of-motion exercises may help prevent further degeneration of the AC joint and reduce the risk of future episodes of pain.
Conclusion
Acromioclavicular joint arthritis is a painful condition that can severely impact a patient’s daily activities, particularly in those who engage in repetitive manual tasks. In this case, a 65-year-old woman found significant relief from an ultrasound-guided AC joint injection. This minimally invasive procedure is an effective treatment option for patients with AC joint arthritis, providing long-term pain relief and improved shoulder function.
By using ultrasound guidance, clinicians can ensure precise needle placement and reduce the risk of complications, making this approach a safe and effective solution for managing shoulder pain due to AC joint arthritis.
Interested to read more about this case and many others? Download NYSORA’s US Pain App!