The analgesic efficacy of a PEC II block
The PEC II block anesthetizes the lateral and medial pectoral nerves, the anterior lateral cutaneous branches of the intercostal nerves, and the intercostobrachialis, providing analgesia for extensive breast surgery, thoracic wall procedures, and sentinel node excision.
Breast cancer surgery remains one of the most effective therapeutic interventions for treating breast cancer. However, this surgery is frequently associated with significant postoperative pain, which can compromise recovery and overall patient experience. This has led to an increasing interest in regional anesthesia techniques as a safer, more effective alternative to systemic analgesia. A new meta-analysis by Versyck et al. 2019 systematically examined the effectiveness of the pectoral type-2 (PEC II) block compared to systemic analgesia alone and the gold-standard thoracic paravertebral block (TPVB). The analysis included 13 randomized controlled trials (RCTs) involving 815 patients undergoing breast cancer surgery.
Key findings
- Reduced opioid consumption:
- The PEC II block significantly reduced opioid consumption in the first 24 hours after surgery compared to systemic analgesia alone.
- Patients receiving the PEC II block used, on average, 13.64 mg less oral morphine equivalents (p < 0.01).
- Postoperative pain scores:
- Patients with the PEC II block experienced significantly lower pain scores at all time intervals within the first 24 hours.
- Pain scores dropped by an average of 1.23 on a 10-point scale, equating to a 39–55% reduction in pain severity.
- Comparable to TPVB:
- The PEC II block showed analgesic efficacy similar to the thoracic paravertebral block.
- There was no significant difference in opioid consumption or pain scores at later postoperative time points.
- Prolonged time to first analgesic request:
- Patients who received the PEC II block delayed their need for the first rescue analgesic by an average of 5 hours compared to systemic analgesia alone.
- No Increase in postoperative nausea and vomiting (PONV):
- Despite the reduction in opioid consumption, no significant reduction in the incidence of PONV was observed in patients receiving the PEC II block.
- Safety profile:
- No major complications were reported with the use of the PEC II block in the reviewed studies, confirming its safety.
Advantages of the PEC II block
- Simplicity and accessibility:
- The PEC II block is easier to administer and less technically challenging than the thoracic paravertebral block.
- It is performed using ultrasound guidance, improving safety and precision.
- Effective analgesia:
- Provides robust pain relief, significantly improving patient comfort in the first 24 hours post-surgery.
- Reduction in opioid use:
- Reduces the need for postoperative opioids, which can minimize opioid-related side effects like sedation, nausea, and respiratory depression.
- Comparable to the gold standard:
- Delivers similar analgesic results as the thoracic paravertebral block without its associated technical complexity.
Clinical implications
The findings highlight the importance of the PEC II block as a viable, effective, and safe analgesic technique for patients undergoing major breast cancer surgery. Given the ongoing concerns surrounding opioid use, regional anesthesia techniques such as the PEC II block offer a significant benefit for postoperative pain management.
Recommendations
- Anesthesiologists should consider incorporating the PEC II block as part of multimodal analgesia for breast cancer surgery.
- Increased focus on training healthcare professionals in ultrasound-guided techniques to improve access and adoption.
- Further studies are needed to assess the long-term benefits, including its impact on chronic post-surgical pain and patient outcomes.
Conclusion
The PEC II block is a powerful analgesic intervention that not only reduces opioid consumption but also delivers comparable efficacy to the technically demanding thoracic paravertebral block. As breast cancer surgeries become more common, the adoption of safer, more effective pain management techniques like the PEC II block could revolutionize postoperative care, leading to improved recovery and patient satisfaction.
For more information, refer to the full article in Anaesthesia.
Versyck B, van Geffen GJ, Chin KJ. Analgesic efficacy of the PEC II block: a systematic review and meta-analysis. Anaesthesia. 2019 May;74(5):663-673.
Here are our 3 go-to tips to perform a PEC II block
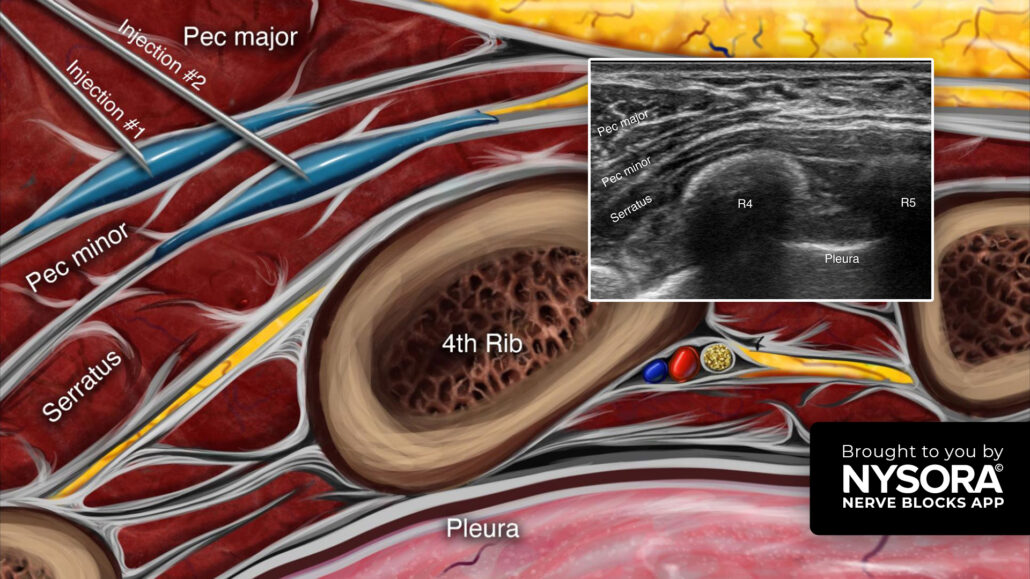
- Place the transducer in a sagittal orientation below the midline of the clavicle.
- From the PEC I position, slide the transducer laterally to identify the 4th and 5th ribs and the serratus anterior muscle.
- Insert the needle in-plane, from anterior to posterior, through the pectoralis major muscle and inject local anesthetic in two fascial planes.
– 10 mL between the pectoralis major and minor muscles (PEC I).
– 15-20 mL between the pectoralis major and serratus anterior muscles (PEC II).
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!