Relationship between injectate volume and spread in Erector Spinae Plane Blocks
The erector spinae plane (ESP) block is a novel interfascial plane technique that was first described in 2016 by Forero et al. The technique is indicated for analgesia for rib fractures and back and chest wall surgeries.
A new study by Gadsden et al. 2024 provides new insights into how the volume of anesthetic injections influences the spread of the anesthetic during erector spinae plane (ESP) blocks. This research aims to enhance our understanding of the block’s mechanism and offer valuable guidance for clinical application.
Background
ESP blocks are increasingly used for pain relief during thoracic and lumbar surgeries. The technique involves ultrasound-guided injection of local anesthetic deep into the erector spinae (ES) muscle plane near the transverse processes of the vertebrae. Compared to other regional anesthesia techniques, ESP blocks have gained popularity because they are perceived as simpler, safer, and more effective.
However, uncertainties remain about the optimal injectate volume and its influence on anesthetic spread. Some clinical and cadaveric studies report variable extents of sensory blockade and nerve involvement, indicating a need for further investigation.
Study objectives and methods
This study explored the relationship between injectate volume and the extent of its cephalocaudal spread in thoracic and lumbar ESP blocks. Researchers also examined whether higher injection volumes might result in spread to unintended areas, such as the paravertebral or epidural spaces.
Key processes included:
- Cadavers: Two unembalmed human cadavers were used to ensure tissue integrity resembling living conditions.
- Injection technique: Ultrasound-guided ESP injections were administered incrementally at thoracic and lumbar levels using a radiographic contrast solution mixed with dye.
- Dissection and imaging: Radiographic imaging and subsequent tissue dissection were performed to evaluate dye distribution and identify any unintended spread.
Results
Spread of injectate:
- Larger injectate volumes resulted in greater cephalocaudal spread, though the increase plateaued at higher volumes.
- For thoracic injections:
- 30 mL spread across 4–7 vertebral levels.
- 60–80 mL extended the spread slightly, reaching up to 9 levels in some cases.
- For lumbar injections:
- 30 mL typically spread across 3–4 levels, with less extensive spread than the thoracic region.
Dye staining during dissection:
- Dye predominantly stained the ventral surface of the ES muscle and dorsal rami.
- No staining was observed in the paravertebral, epidural, or pleural spaces, regardless of volume.
- Larger volumes showed lateral and dorsal staining but failed to reach ventral rami or anterior structures.
Lack of unintended spread:
- Even with high injectate volumes (up to 80 mL), there was no evidence of spread to critical areas like the pleura, epidural, or paravertebral space. This confirms the safety of ESP blocks in avoiding these regions.
Clinical implications
The findings provide guidance for clinicians performing ESP blocks:
- Optimal volume: A single injection of 30 mL offers effective analgesia across 4–7 thoracic levels and 3–4 lumbar levels, making it suitable for most surgical procedures.
- Higher volumes: Larger injectate volumes (60–80 mL) may benefit patients requiring broader analgesic coverage, though the increase in spread is marginal beyond 60 mL.
- Safety: The study reassures practitioners about the minimal risk of unintended anesthetic spread, even with high injection volumes.
Study limitations
While the findings are promising, the study’s cadaveric nature presents limitations:
- Differences in tissue compliance, temperature, and pressure between cadavers and living patients may affect anesthetic spread.
- The use of dye and radiographic contrast, rather than actual anesthetic agents, may limit the generalizability of results to clinical settings.
- Findings from only two cadavers require validation through larger studies with live subjects.
Conclusion
This study advances our understanding of the relationship between injectate volume and anesthetic spread in ESP blocks. It highlights the effectiveness of 30 mL for routine clinical use and reassures practitioners about the safety of larger volumes in avoiding critical areas.
For more information, refer to the full article in Regional Anesthesia & Pain Medicine.
Gadsden J, Gonzales J, Chen A. Relationship between injectate volume and disposition in erector spinae plane block: a cadaveric study. Reg Anesth Pain Med. 2024 Jul 8;49(7):511-517.
Let’s outline 3 key steps for a successful ESP block procedure:
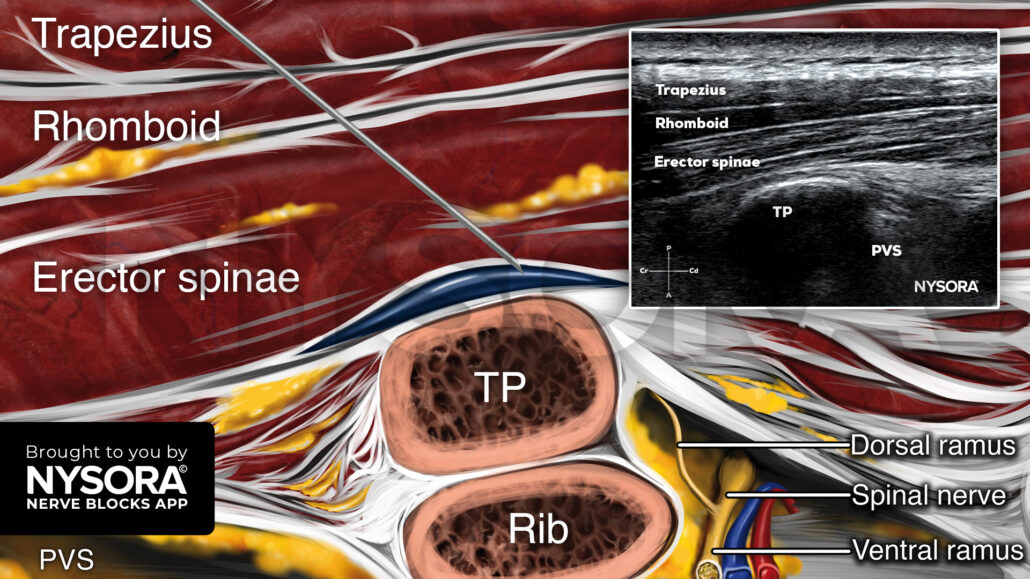
- Select the target transverse process and place the transducer in a paramedian sagittal orientation, approximately 2 cm away from the midline.
- Identify the following structures on ultrasound: All 3 layers of the ESP muscles, the rib-transverse process complex of interest, and the paravertebral space. The pleura should not be visualized.
- Insert the needle in-plane, from cranial to caudal, and inject 20-30 mL of local anesthetic in the plane deep to the ESP muscles and superficial to the transverse processes to achieve a craniocaudal distribution along several vertebral levels.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!