
Learning objectives
- Diagnose and treat lithium toxicity
Definition and mechanisms
- Lithium is a very powerful, antimanic medication with a narrow therapeutic index
- Excessive intake or impaired excretion can result in lithium accumulation
- Decreased excretion may occur as a result of dehydration such as from vomiting or diarrhea, a low sodium diet, or from kidney problems
- Co-ingestants can increase the risk of lithium toxicity
- NSAIDs
- Indomethacin
- Selective COX-2inhiitors
- Acetaminophen
- Metronidazole
- Calcium channel blockers
- ACE inhibitors
- Diuretics
- Acute toxicity: lithium overdose in a patient who does not regularly take lithium
- Acute-on-chronic toxicity: acute overdose in a patient who takes lithium daily, a sudden decline in renal function in a patient taking lithium can also lead to acute-on-chronic toxicity
- Chronic toxicity: the history generally involves a patient on chronic lithium therapy who, due to toxic drug effects, physical disability, or concurrent illness, becomes hypovolemic, leading to reduced renal excretion of lithium alternatively and toxicity can develop solely from the effects of medications that reduce kidney function
Signs and symptoms
- Mild symptoms occur at a level of 1.5-2.5 mEq/L
- Nausea and fatigue
- Moderate symptoms occur at a level of 2.5-3.5 mEq/L
- Confusion, increased heart rate, and low muscle tone
- Severe symptoms occur at a level > 3.5 mEq/L
- Coma, hypotension, and increased body temperature
| Neurological effects | Tremor Hyperreflexia Nystagmus Ataxia Confusion Delirium |
| Renal effects | Renal toxicity Impaired urinary concentrating ability Nephrogenic diabetes insipidus Sodium-losing nephritis Nephrotic syndrome |
| Cardiovascular effects | T wave flattening Sinus node dysfunction QT prolongation Intraventricular conduction defects U waves |
| Gastrointestinal effects | Nausea Vomiting Diarrhea Abdominal pain |
| Endocrine effects | Hypothyroidism |
Complications
- Cerebellar dysfunction
- Extrapyramidal symptoms
- Brainstem dysfunction
- Memory deficits
- Cognitive deficits
- Sub-cortical dementia
Diagnosis
- Lithium levels > 1.2 mEq/L
- ECG
- Fingerstick glucose
- Renal function
- Serum acetaminophen and salicylate concentrations
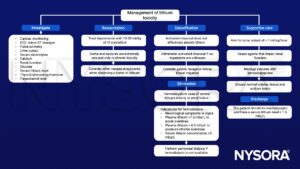
Management
Anesthetic implications
- Lithium prolongs both depolarizing and non-depolarizing neuromuscular block
- Perform neuromuscular monitoring in patients on lithium undergoing general anesthesia with the use of neuromuscular blocking agents
- Consider conduction defects and ST changes on ECG in patients on lithium undergoing GA
Suggested reading
- Gitlin, M., 2016. Lithium side effects and toxicity: prevalence and management strategies. International Journal of Bipolar Disorders 4.
- Flood S, Bodenham A. 2010. Lithium: mimicry, mania, and muscle relaxants. Continuing Education in Anaesthesia Critical Care & Pain. 10;3:77–80.
We would love to hear from you. If you should detect any errors, email us customerservice@nysora.com











