
Learning objectives
- Diagnose and treat intoxication with the toxic alcohols methanol and ethylene glycol (EG)
Background
- EG is a common component of antifreeze and de-icing solutions
- Methanol is present as a solvent in many household products, such as antifreeze, cleaning solutions, dyes, and paint removers
- Onset of symptoms of methanol poisoning can range from 40 minutes to 72 hours, depending on the dose and co-ingestion of ethanol
Pathophysiology
- Toxicity of methanol and EG is related to the production of toxic metabolites by the hepatic enzyme alcohol dehydrogenase (ADH)
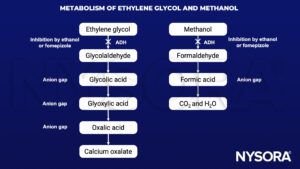
- Oxalic acid
- The main toxic metabolite of EG
- Binds to calcium, forming insoluble calcium oxalate crystals, this can cause hypocalcemia and crystal deposition in several organs causing organ dysfunction
- Formic acid
- The main toxic metabolite of methanol
- Directly toxic to the retina which can cause visual disturbances and even blindness
- Inhibits the mitochondrial cytochrome oxidase, which deranges ATP synthesis
Signs and symptoms
| Ethylene glycol | Methanol | |
|---|---|---|
| Early | Confusion Stupor Nausea Vomiting | Mild euphoria Drunkenness Headache Lethargy Confusion |
| Progression | Metabolic acidosis Küssmaul breathing Hypocalcemia Hyperreflexia | Vision abnormalities Extrapyramidal symptoms (in severe intoxication) Seizures Metabolic acidosis Küssmaul breathing |
| Late | Coma Acute renal failure (earlier in severe intoxication) Cardiovascular shock Multi organ failure Death | Blindness Coma Cardiovascular shock Respiratory failure Sudden respiratory arrest Death |
Management
- Decreased consciousness
- Requires endotracheal intubation if airway is at risk
- Administer a pre-intubation bolus of 1-2 mmol/kg sodium bicarbonate to avoid exacerbating acidosis, which will worsen symptoms
- Supportive care
- IV fluids
- Vasopressors as needed
- Correct acidemia (pH<7.3) by administering sodium bicarbonate
- Supplement calcium in EG intoxication
- Decontamination
- Activated charcoal and gastric lavage have no place in the treatment of toxic alcohol intoxication
- Seizures
- Treat with a benzodiazepine
- Antidotal therapy:
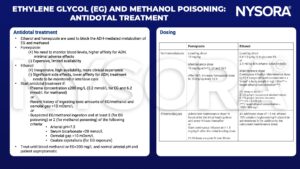
- Hemodialysis
- Start hemodialysis if
- Methanol/EG intoxication with: Coma, convulsions, renal failure, metabolic acidosis pH<7.15, persisting acidosis despite treatment or serum anion gap>24 mmol/L
- Plasma concentration ≥500 mg/L if not yet antidotal treatment, ≥600 mg/L if ethanol, ≥700 mg/L if fomepizole
- Start hemodialysis if
Suggested reading
- Rietjens SJ at al. Ethylene glycol or methanol intoxication: which antidote should be used, fomepizole or ethanol? Neth J Med. 2014 Feb;72(2):73-9. PMID: 24659589
- Grouls R. et al. Toxicologie behandel informatie: Methanol, 2022, accessed 25/01/2023 https://toxicologie.org/methanol
We would love to hear from you. If you should detect any errors, email us customerservice@nysora.com






