NYSORA Volume 10 March 2009
The aim of this study was to test the clinical utility of the lateral approach to popliteal block and compare its effectiveness and patient acceptance to that of the posterior approach.
|
Significance
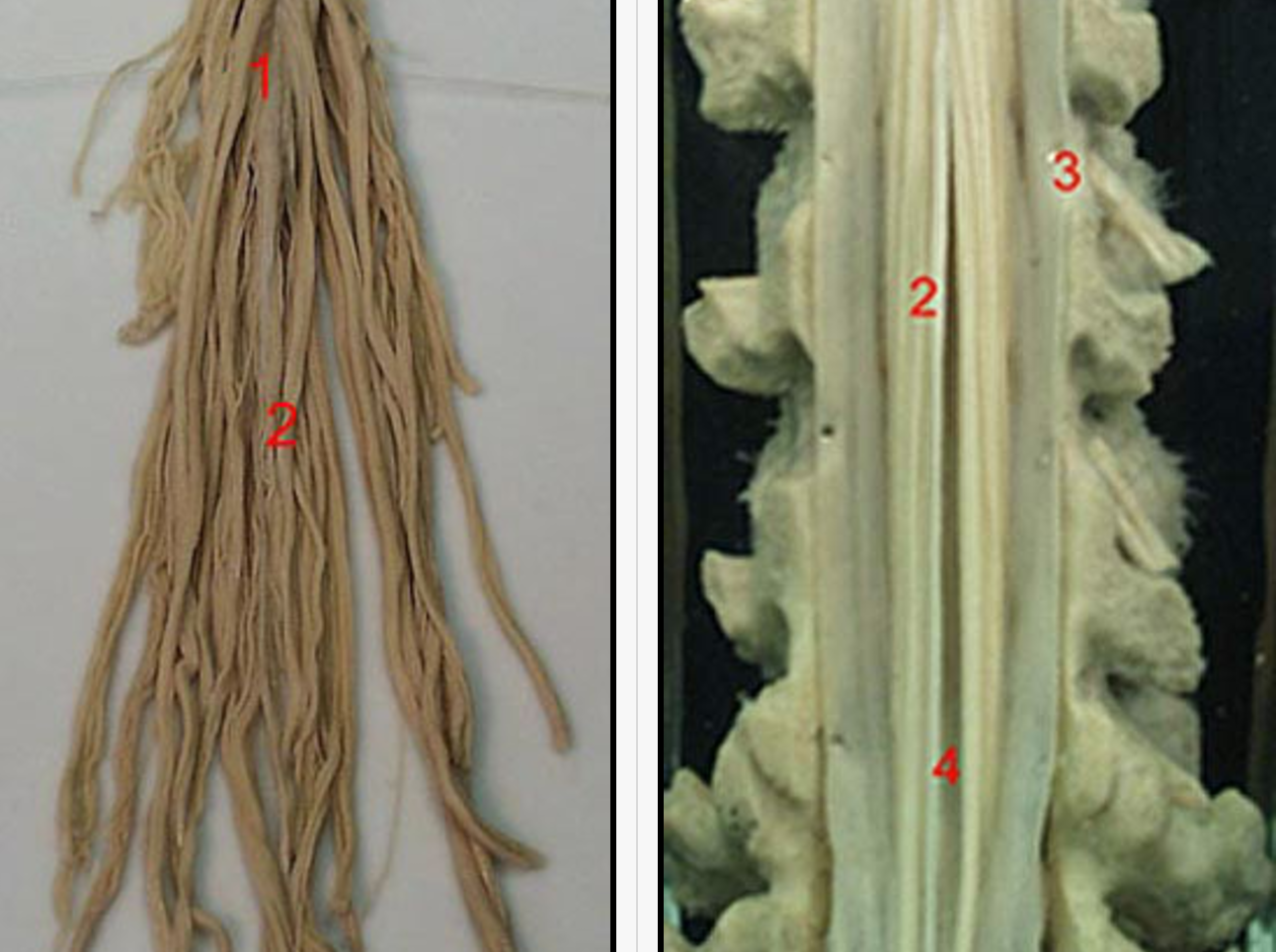
Figure 1. A cadaveric model for the lateral approach to popliteal block: A cross-sectional anatomy of the popliteal fossa. The sloped lines represent two different angles of needle insertion. Circles represent injectates at 30 degree angle and squares injectates at 60 degree angle. The need to position the patient in the prone position is the main disadvantage of the posterior approach to the sciatic nerve block in the popliteal fossa (popliteal block). This may preclude the use of the popliteal block in patients who could benefit the most from this technique (i.e. advanced pregnancy, morbid obesity, spine and hemodynamic instability, mechanical ventilation). A recent study in a human cadaver model demonstrated that the sciatic nerve in the popliteal fossa can also be reliably accessed in the supine position using the lateral approach, Figure 1 (1). A needle inserted seven cm above the knee in the groove between the biceps femoris and vastus lateralis muscles, and advanced at a 30 degree downward angle relative to the horizontal plane, resulted in a reliable approximation of the needle tip to the popliteal nerve. While the study in cadavers provided guidance for the design of the lateral approach to the popliteal block, its ease and effectiveness has not yet been examined in clinical practice. The aim of this study was to test the clinical utility of the lateral approach to popliteal block and compare its effectiveness and patient acceptance to that of the posterior approach. Methods Fifty patients undergoing lower leg surgery were randomized to receive a popliteal block using either the lateral or the posterior approach. All patients received midazolam 10 to 30 µcg/kg and fentanyl 1 to 2 µcg/kg intravenously prior to introduction of the anesthetic. Additional doses of midazolam and fentanyl in increments of 1 mg and 50 µcg, respectively, were administered as necessary during the block performance and surgery, in order to allay any accompanying anxiety and discomfort. The nature and exact origin of the discomfort were elicited from the patients before any additional sedatives or analgesics were given. When it was determined that patients experienced pain on surgical instrumentation, additional infiltration with a local anesthetic by the surgeon was implemented or an alternative anesthetic was considered.  Figure 2: A 100 mm long stimulating needle is inserted in a horizontal plane between the biceps femoris and the vastus lateralis muscles until the femur is contacted. Technique Of The Popliteal Block Using The Lateral Approach:
 Figure 3. The needle is inserted posteriorly at a 30 degree angle to the horizontal plane. Technique Of The Popliteal Block Using The Posterior Approach:
While the techniques of the popliteal block differed between the lateral and posterior approach, the preparation for the block, local anesthetic solution used for the blocks, and the technique of nerve stimulation were similar. In both techniques the following procedure was followed:
The data collected included: patient demographics, time from the first needle insertion to successful nerve localization (time required for performance of the block), number of attempts to localize the popliteal nerve (defined as a number of skin punctures). The presence of sensory block in the distribution of the peroneal and tibial nerves was ascertained using the pinprick method every 5 minutes following injection of the local anesthetic, for up to 30 minutes. The presence of motor block was assessed by testing the ability of the patient to perform plantar or dorsal flexion of the foot 30 minutes following the injection. A successful block was defined as a complete sensory block affecting both divisions of the sciatic popliteal nerve within 30 minutes and absence of pain on surgical instrumentation. Surgery proceeded once sensory anesthesia in the surgical field was documented by pinching the skin by the surgeon using a hemostat clamp. Postoperative pain assessments were performed by postanesthesia care unit (PACU) nurses blinded to the purpose of the study. Patients were assessed every 15 minutes from the time of admission to PACU (Phase 1 recovery) until their discharge home or transfer to the floor. The time to the first administration of analgesics was evaluated only among inpatients, since the data could not be reliably obtained in all patients who were discharged to their homes. All patients were interviewed by an anesthesiologist (blinded to the popliteal block technique) in person (inpatients) or by telephone (outpatients) 24 hours after the operation. During the interview, patients’ responses to questions relating to discomfort and pain during block placement, and satisfaction with anesthesia technique were recorded. Pain and discomfort during block placement were rated as: no pain, slightly painful, moderately painful, painful and extremely painful. Patient satisfaction with the anesthetic technique was assessed by questioning as to whether they would choose the same anesthesia technique for any eventual subsequent surgery, or if they would recommend the popliteal block technique to their friends. Statistical Analyses Data are presented as mean +/- standard deviations for continuous variables and as counts and percentages for nominal data. Differences between patients receiving the posterior or the lateral approach with respect to continuous variables (age, height, weight, intensity of the stimulating current, time to complete the block, time to surgical incision, duration of operation) were tested by Student’s t-test for independent samples. Differences in proportions of patients in the two groups with respect to nominal data (sex, type of surgery, inpatient vs. ambulatory surgery, number of attempts, number of successes) were tested by P 2, or by Fisher’s exact test when numbers were small. Discomfort was assessed by a P 2 for trend. All analyses were performed using the Statistical Package for the Social Sciences (SPSS for Windows), version 5.02 (Chicago, IL, 1993). Differences were considered significant at the 0.05 level. Results Fifty patients were enrolled in the study. There were no significant diferences in demographics (age, weight, height), ASA status, or type of surgical procedure between the groups (Table 1 ).
There were no significant differences in demographics, surgical procedures or the use of tourniquets between patients receiving the popliteal block through the posterior or through the lateral approach. Legend: TMTA-trans-metatarsal amputation, I&D-incision and drainnage, ORIF-open reduction and internal fixation, BKA-below knee amputation. Both techniques resulted in successful block in all but one patient in the lateral approach group, who underwent transmetatarsal amputation of the foot. Despite adequate anesthesia on assessment, bone incision proved to be painful, which required infusion of propofol (100-130 microgram/kg/min) for completion of the procedure. On admission to PACU, however, the patient had a full sensory and motor block, and did not require any analgesics for 630 minutes after surgery. The time to the first analgesic in the posterior PNB group was 568 +/- 159 minutes (range 320-760 min) and 595 +/- 133 minutes (range 365-780 min) in the lateral PNB group; p> 0.05. Five saphenous nerve blocks (two in the posterior and three in the lateral group) were judged as having failed. Although these patients required supplemental injections of local anesthetics in the distribution of the saphenous nerve, as well as additional doses of intravenous midazo-MTA- trans-metatarsal amputation, I&D-incision and drainnage, ORIF-open reduction and internal fixation, BKA-below knee amputation. Both techniques resulted in successful block in all but one patient in the lateral approach group, who underwent transmetatarsal amputation of the foot. Despite adequate anesthesia on assessment, bone incision proved to be painful, which required infusion of propofol (100-130 microgram/kg/min) for completion of the procedure. On admission to PACU, however, the patient had a full sensory and motor block, and did not require any analgesics for 630 minutes after surgery. The time to the first analgesic in the posterior PNB group was 568 +/- 159 minutes (range 320-760 min) and 595 +/- 133 minutes (range 365-780 min) in the lateral PNB group; p> 0.05. Five saphenous nerve blocks (two in the posterior and three in the lateral group) were judged as having failed. Although these patients required supplemental injections of local anesthetics in the distribution of the saphenous nerve, as well as additional doses of intravenous midazolam, propofol or fentanyl, none of them required induction of an alternative anesthetic. There was no difference in the popliteal block success rate between the two techniques. However, while the majority of patients in the posterior group required only one or two attempts, the majority of patients in the lateral group required a third or fourth attempt in order to localize the nerve (Table 2). This difference was statistically significant (p < 0.001). The initial response to nerve stimulation also significantly varied between the two techniques, with stimulation of the common peroneal nerve being the most common first response (72%) in the lateral approach group, and the tibial nerve response being the most common (76%) in the posterior approach group (Table 2).
Only two patients required pain medication prior to discharge home (104 and 140 minutes after block placement). Both patients, ametatarsal amputation and a procedure on the medial ankle respectively, complained of pain in the medial aspect of the foot with persistant motor block of the foot. The stimulus intensity required for nerve localization, did not show any signifficant difference between the groups, with the majority of patients requiring a current of 0.4 mA, (Table 2).While the majority of patients reported only minimal or no pain during needle insertion (Table 3). During telephone interviews, all patients expressed high satisfaction with both techniques, and stated that they would choose it for any eventual, subsequent surgery, and would recommend it to their friends.
Discussion The lateral approach to the popliteal block consistently provided reliable surgical anesthesia in the distribution of both divisions of the sciatic nerve. The lateral technique allowed performance of the popliteal block block with patients in the supine position, with the onset and quality of anesthesia, as well as patient comfort during block placement comparable to that of the posterior approach. Consistent with our previous report in human cadavers [1], the lateral approach to popliteal block in patients resulted in a predictable approximation of the needle tip to the popliteal nerve. While the lateral approach differed from the posterior in regard to patient positioning, anatomical landmarks and the technique of block performance, the current requirements and principles of nerve localization were similar. Of note, the common peroneal nerve was stimulated more frequently through the lateral than through the posterior approach. This is not surprising, since the peroneal nerve is located laterally, Figure 4. Additionally, the lateral approach required a greater number of attempts and slightly longer time for block completion. One possible contributing factor was the lack of experience with the new technique. A 100 mm long 21G needle used in the lateral technique tended to bend on insertion more than the 50 mm long 22G needle used in the posterior approach, which possibly contributed to the longer time to nerve localization. A shorter needle (e.g., 70 mm), or a needle of a larger diameter (e.g., 20G) could result in a more consistent needle path, and therefore might be preferable for the lateral approach. While it is possible that the lateral approach might be associated with a somewhat greater patient discomfort due to the needle passage through the biceps and/or vastus lateralis muscles (tendons), as well as a larger diameter of the needle, this was not observed under conditions of this study. The premedication with midazolam, and local infiltration of the skin with local anesthetic may have altered the patients perception of pain, making it difficult to discern any differences in discomfort during block performance. Local contractions of the biceps femoris muscle, frequently observed during needle advancement, provided a useful estimate of the required depth of needle insertion in the lateral approach to the popliteal block. Since at this level the sciatic nerve is located close to the medial aspect of the biceps femoris muscle (Figure 4), stimulation of the nerve was usually obtained with further advancement of the needle 3 to 5 mm after the local twitches of the biceps femoris muscle disappeared. Failure to localize the nerve with further needle advancement after cessation of the twitches of the biceps femoris muscle indicates that the plane of needle insertion is either anterior or posterior to the nerve. In this case, the needle should be withdrawn to the skin and reinserted with a slight anterior or posterior angulation. The use of a higher initial stimulating current (about 0.8 mA) was beneficial during nerve localization through the lateral approach by accentuating the local contractions of the biceps femoris muscle, which served as an additional guide during block placement. Although use of the popliteal block in clinical practice has many potential advantages over neuraxial techniques in patients undergoing lower extremity surgery (5), the technique is infrequently utilized by anesthesiologists in the United States (6). In addition to unfavorable local practice settings (7), possible explanations for infrequent clinical use of the popliteal block include inadequate exposure to this technique during residency training (7), as well as the inability of patients to lie in the prone position, mandated in the popliteal block using a posterior approach (2,8). Another technique of the lateral approach to the popliteal block (9,10) described the use of the procedure for postoperative pain management. The technique involved inserting a needle horizontally, anterior to the tendon of the biceps femoris muscle, with the leg slightly flexed in the knee joint, on a pillow. Although this technique provided good postoperative pain relief in patients after foot surgery, its frequent failure to provide adequate analgesia (9,10) makes it unsuitable for surgical anesthesia. The high success rate of the popliteal block in our study is likely the result of precise nerve localization using low intensity nerve stimulation ( In summary, the lateral approach popliteal block for ankle and foot surgery resulted in reliable anesthesia, comparable to that of the popliteal block using the posterior approach. The performance of the block using the lateral approach appeared straightforward when the described technique was followed, although it took more attempts at nerve localization. In addition to using the popliteal block in patients who can not assume the prone position, this technique provides the option of performing supplementary blocks (i.e., saphenous or femoral nerve blocks) and surgery without the need for patient repositioning. REFERENCES: 1. Vloka JD, Hadzic A, Kitain E, Lesser JB, Kuroda MM, April EW, Thys DM. Anatomic considerations for sciatic nerve block in the popliteal fossa through the lateral approach. Reg Anesth 1996;21:414-418. 2. Singelyn FJ, Gouverneur JM, Gribomont BF. Popliteal sciatic nerve block aided by a nerve stimulator: a reliable technique for foot and ankle surgery. Reg Anesth 1991;16:278-81. 3. Vloka JD, Hadzic A, Singson R, Koorn R, Thys DM. The popliteal nerve block revisited: Results of an MRI study. Anesth Analg 1997;84:S344. 4. Rorie DK, Byer DE, Nelson DO, Sittipong R, Johnson KA . Assessment of block of the sciatic nerve in the popliteal fossa. Anesth Analg 1980;59:371-6. 5. Vloka JD, Hadzic A, Mulcare R, Lesser JB, Koorn R, Thys DM. Combined blocks of the sciatic nerve at the popliteal fossa and posterior cutaneous nerve of the thigh for short saphenous vein stripping in outpatients: An alternative to spinal anesthesia. J Clin Anesth 1997;9:618-22. 6. Hadzic A,Vloka JD, Kuroda MM, Koorn R, Birnbach DJ, Thys DM. The use of peripheral nerve block in anesthesia practice. A national survey. Anesth Analg, 1997;84:S300. 7. Kopacz DJ, Bridenbaugh LD. Are anesthesia residency programs failing regional anesthesia? The past, present, and future. Reg Anesth 1993;18(2):84-7. 8. Adriani J. Labat’s Regional Anesthesia. Techniques and Clinical Applications. Philadelphia, PA, W.B. Saunders Company 1967, pp 317-21. 9. McLeod DH, Wong DHW, Claridge RJ, Merrick PM. Lateral popliteal sciatic nerve block compared with subcutaneous infiltration for analgesia following foot surgery. Can J Anaesth 1994;41(8):673-6. 10. McLeod DH, Wong DHW, Vaghadia H, Claridge RJ. Lateral popliteal sciatic nerve block compared with ankle block for analgesia following foot surgery. Can J Anaesth 1995;42 (9):765-9. 11. Braun DL. Popliteal block. In Atlas of regional anesthesia. 1st eddition. W.B. Saunders 1992, pp 109-13. 12. Vloka JD, Hadzic A, Lesser JB, Kitain E, Geatz H, April EW, Thys DM. A Common Epineural Sheath for the Nerves in the Popliteal Fossa and Its Possible Implications for Sciatic Nerve Block. Anesth Analg 1997;84:387-90. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||