
Explore NYSORA knowledge base for free:
Explore NYSORA knowledge base for free:



NYSORA Ultrasound-Guided Pain Blocks App describes the most practical and applicable techniques of ultrasound-guided pain medicine

Gain access to the most comprehensive guide on US-guided chronic pain interventions, including: Spine Injections, Abdominal and Pelvic Blocks, Peripheral Nerve Blocks, Diagnostic and Musculoskeletal Ultrasound, Diagnostic Neurosonology, Joint Injections, Nerve Blocks, Interventional Headache Treatment, Stimulation Procedures and more…
Subscribe and get full access! With annual subscription subscribers will receive a proof of payment for education reimbursement. You also save 15% if you choose the annual subscription instead of monthly!
Join the community of over 30,000 professionals worldwide and see for yourself why NYSORA’s US-Guided Interventional Pain APP is the first and the most authoritative guide to ultrasound and nerve blocks.


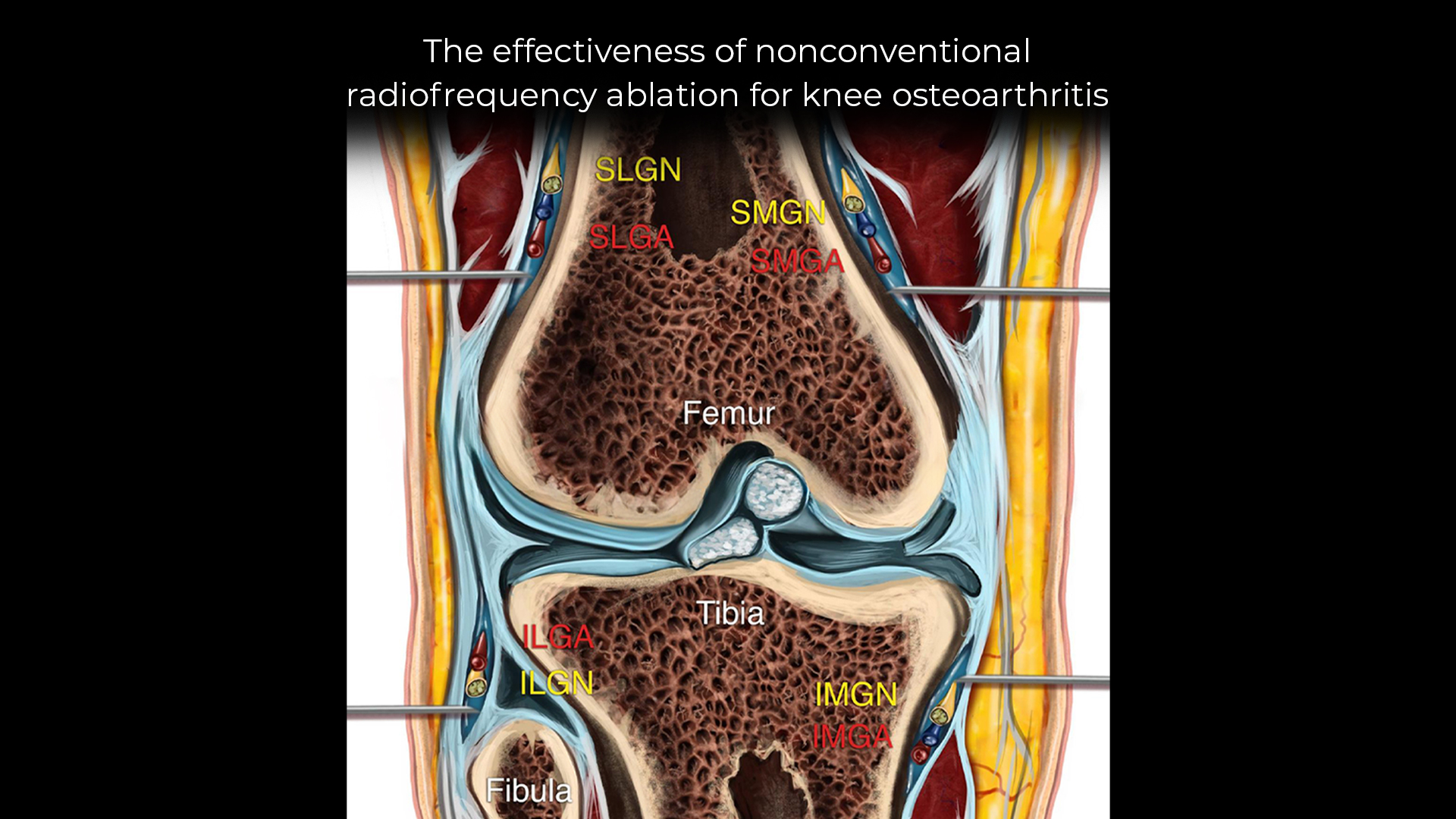
Knee osteoarthritis (OA) is a common, degenerative joint condition that leads to chronic pain and functional limitations. While conventional treatments such as physiotherapy, medications, and surgery offer temporary relief, more advanced pain management options like radiofrequency ablation (RFA) have shown promising results. This article delves into the effectiveness of nonconventional RFA techniques—specifically pulsed and cooled RFA—targeting the genicular nerves for knee OA pain management based on recent research findings. What is radiofrequency ablation? Radiofrequency ablation (RFA) is a minimally invasive procedure that uses thermal energy to disrupt nerve signaling, thereby reducing pain. The technique has evolved, with pulsed and cooled RFA emerging as alternatives to the traditional high-temperature probe method. These newer techniques minimize damage to surrounding tissues while offering long-lasting pain relief. Cooled RFA: This method pumps water inside the probe to maintain lower temperatures (60°C – 70°C) while targeting larger areas of neuronal tissue. This reduces thermal damage to surrounding tissues, leading to prolonged pain relief. Pulsed RFA: Pulsed RFA uses intermittent high-voltage bursts to limit tissue heating (maximum 42°C), thus preventing permanent nerve damage. This technique reduces the risk of complications and may provide reversible pain relief. Meta-analysis study: Evaluating effectiveness A recent meta-analysis by Soetjahjo et al. (Pain Physician, 2024) examined the effectiveness of pulsed and cooled RFA in treating knee OA pain. The study included 11 publications and assessed both pain relief and physical function improvement. Key findings Pain reduction: Both cooled and pulsed RFA led to significant pain reduction at 1, 3, and 6 months post-procedure. There was no significant difference in pain relief between the two techniques. Physical function: Pulsed RFA showed greater improvement in physical function at the 1-month and 3-month follow-ups, while cooled RFA did not demonstrate significant functional gains. Adverse effects: Few adverse effects were reported, primarily minor issues such […]

Preoperative pain sensitivity (PPS) is increasingly recognized as a significant factor in predicting postoperative pain outcomes. According to a 2024 systematic review and meta-analysis published in the British Journal of Anaesthesia, PPS has notable correlations with both acute and chronic postoperative pain. The findings from this study provide insights into how pain thresholds before surgery can inform the management of postoperative pain, especially in high-risk patients. What is preoperative pain sensitivity (PPS)? Preoperative pain sensitivity refers to how individuals perceive and tolerate pain before surgery. This sensitivity can be evaluated using various methods, such as: Quantitative Sensory Testing (QST): Includes methods like pressure, heat, and electrical pain thresholds. Pressure Pain Threshold (PPT): Measures the minimum pressure that causes pain. Electrical Pain Threshold (EPT): Measures pain in response to electrical stimulation. Temporal Summation of Pain (TSP): Assesses how pain increases with repeated stimuli. Pain Sensitivity Questionnaire (PSQ): A self-reported tool where patients rate the perceived intensity of everyday painful situations. Key findings The meta-analysis included 70 prospective observational studies with over 8,300 patients, evaluating the correlation between PPS and postoperative pain. The results provide a foundation for developing tailored pain management strategies. Key takeaways from the study include: Lower pressure and electrical pain thresholds (PPT, EPT) before surgery are linked to increased acute postoperative pain. Higher temporal summation of pain (TSP) is associated with both acute and chronic postoperative pain. PSQ was only linked to acute postoperative pain but showed no significant association with chronic pain. Acute vs. chronic postoperative pain The study highlights the different mechanisms behind acute and chronic postoperative pain: Acute pain: Most strongly linked with preoperative pressure and electrical pain thresholds. Chronic pain: Only TSP shows a significant correlation, emphasizing its role in the long-term management of postoperative discomfort. Why preoperative pain sensitivity matters in postoperative pain […]
Adhesive capsulitis, more commonly known as frozen shoulder, is a debilitating condition that causes pain, stiffness, and a significant loss of shoulder mobility. For many patients, traditional treatment methods can be slow to bring relief, and the journey to recovery is often fraught with setbacks. However, a novel ultrasound-guided approach, known as the Saline Hydrodistension of the Anterior Capsular (SHAC) technique, is emerging in the treatment of this condition. Understanding adhesive capsulitis Adhesive capsulitis is characterized by the formation of excessive scar tissue within the shoulder joint, leading to painful restriction of movement. The condition can be primary, occurring spontaneously, or secondary, often following trauma, surgery, or other underlying health conditions. Patients with this condition typically endure months of pain and a gradual loss of both active and passive range of motion. What is the SHAC technique? The SHAC technique represents a significant advancement in the management of adhesive capsulitis. This procedure involves the precise injection of saline and steroids into the anterior capsular space of the shoulder joint under ultrasound guidance. Unlike more traditional methods, such as posterior or rotator interval approaches, the SHAC technique offers targeted pain relief and allows for immediate mobilization of the shoulder post-procedure. How does the SHAC technique work? Anatomy and access points The SHAC technique leverages specific anatomical landmarks within the shoulder joint: Fascial sheaths: The procedure targets the fascial sheath between the deltoid and subscapularis muscles, as well as the sheath beneath the subscapularis myotendinous junction. These sheaths provide optimal access to the glenohumeral joint. Foramen of Weitbrecht: Located between the superior and middle glenohumeral ligaments, this foramen allows entry into the intra-articular space. Foramen of Rouviere: Another access point, located between the middle and inferior glenohumeral ligaments, offers an alternative route into the joint. The procedure The SHAC technique is performed […]
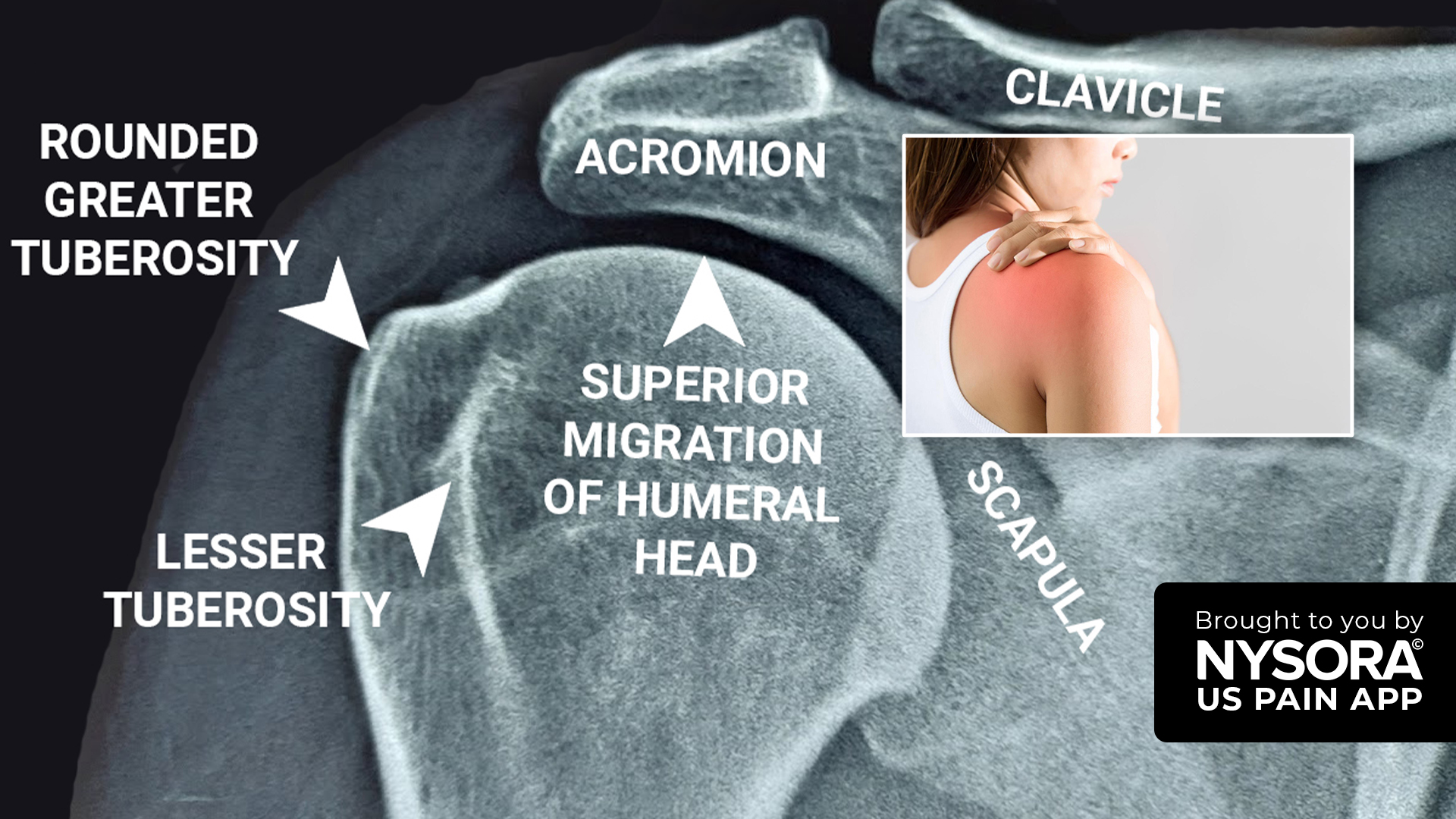
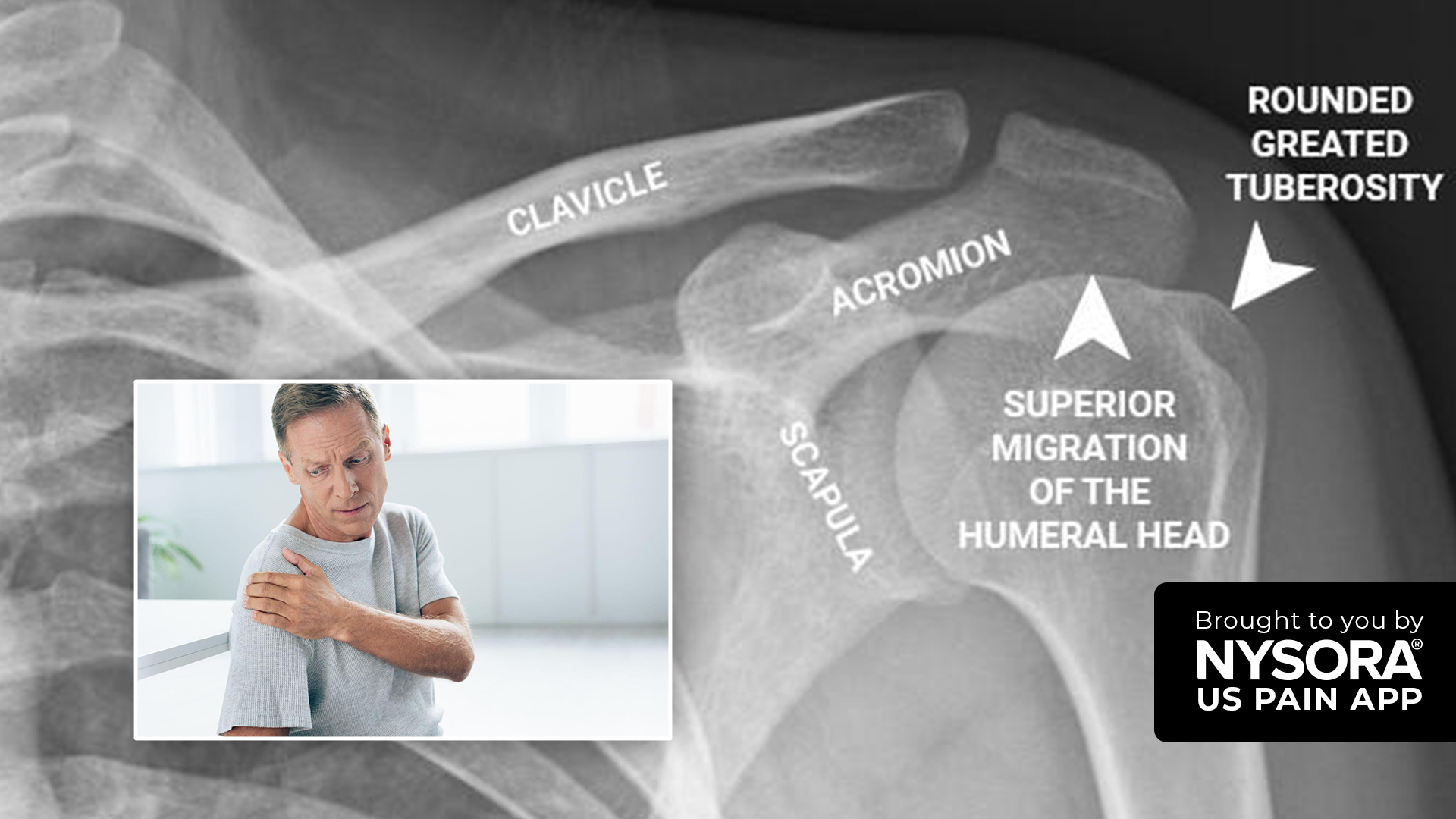
Case Presentation A 56-year-old diabetic woman presents with a two-year history of increasing right shoulder pain, stiffness, night pain, and upper limb swelling, significantly impacting her ability to perform household tasks. Diagnosis Physical Exam Findings Painful shoulder abduction Painful external rotation Painful arc present Positive O’Brien’s Test Clinical Observations Edematous right upper limb Shiny, pale, and cold skin, suggestive of complex regional pain syndrome (CRPS) Laboratory and Imaging Studies Fasting Blood Sugar: 188 mg% Hemoglobin A1c: 9.0% Normal ESR and CRP Normal Nerve Conduction Study and Doppler X-ray: Rotator cuff arthropathy Ultrasound: Rotator cuff tendinopathy, supraspinatus tendinopathy Final Diagnosis Adhesive Capsulitis (Frozen Shoulder) Rotator Cuff Tendinopathy Complex Regional Pain Syndrome (CRPS) CRPS Diagnosis Budapest Criteria To diagnose CRPS, the patient must have at least one symptom in three of the following categories and one sign in two or more categories: Symptoms: Sensory: Hyperesthesia, allodynia Vasomotor: Temperature asymmetry, skin color changes Sudomotor/Edema: Edema, sweating changes Motor/Trophic: Decreased range of motion, motor dysfunction, trophic changes Signs: Sensory: Hyperalgesia, allodynia Vasomotor: Skin temperature asymmetry, skin color changes Sudomotor/Edema: Edema, sweating changes Motor/Trophic: Decreased range of motion, motor dysfunction, trophic changes CRPS Overview Complex Regional Pain Syndrome (CRPS) is a chronic pain condition affecting one limb, often after injury. Symptoms include severe pain, sensitivity to touch, temperature changes, skin color changes, and swelling. Early diagnosis and intervention are crucial. Treatment includes physical therapy, pain medications, nerve blocks, and psychological support. Conclusion Understanding and diagnosing CRPS early is vital for managing symptoms effectively. Proper clinical evaluation and diagnostic criteria, such as the Budapest Criteria, are essential for accurate diagnosis. For more detailed information on CRPS and how Dr. Madhan Pandian treated this patient, download NYSORA’s US Pain app!
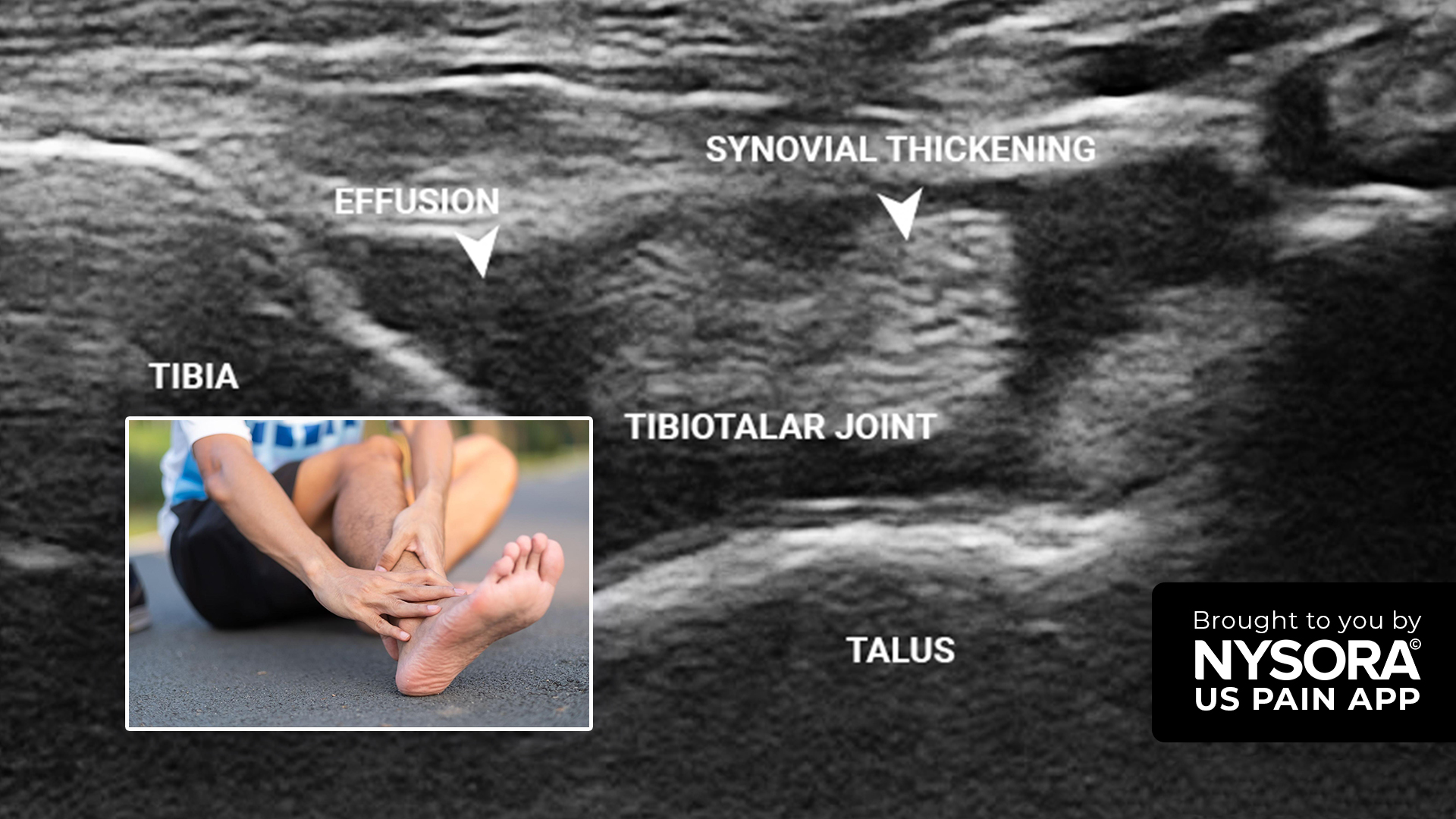
A 20-year-old man developed mild to moderate ankle pain after dancing. He has flat feet but no history of previous injuries. Although non-steroidal anti-inflammatory drugs (NSAIDs) provide him temporary relief, his pain keeps returning and has been worsening over the past month. Physical examination Medial and anterior ankle pain Dorsal foot pain No heel or Achilles pain No increase in pain on provocative maneuvers No edema or redness No tenderness Bilateral pes planus Ultrasound findings Synovial thickening and effusion in the tibiotalar joint Posterior tibial joint tenosynovitis Diagnosis The patient was diagnosed with ankle joint effusion and posterior tibial tendinopathy. Ankle joint effusion, often referred to as a swollen ankle, involves the accumulation of excess fluids in the soft tissues surrounding the joint. This condition frequently results from infection, inflammation, trauma, or overuse. Read more about the treatment, patient outcome, and other case studies in the US Pain App. Ready to elevate your knowledge? Tap HERE to download the go-to app for chronic pain procedures.
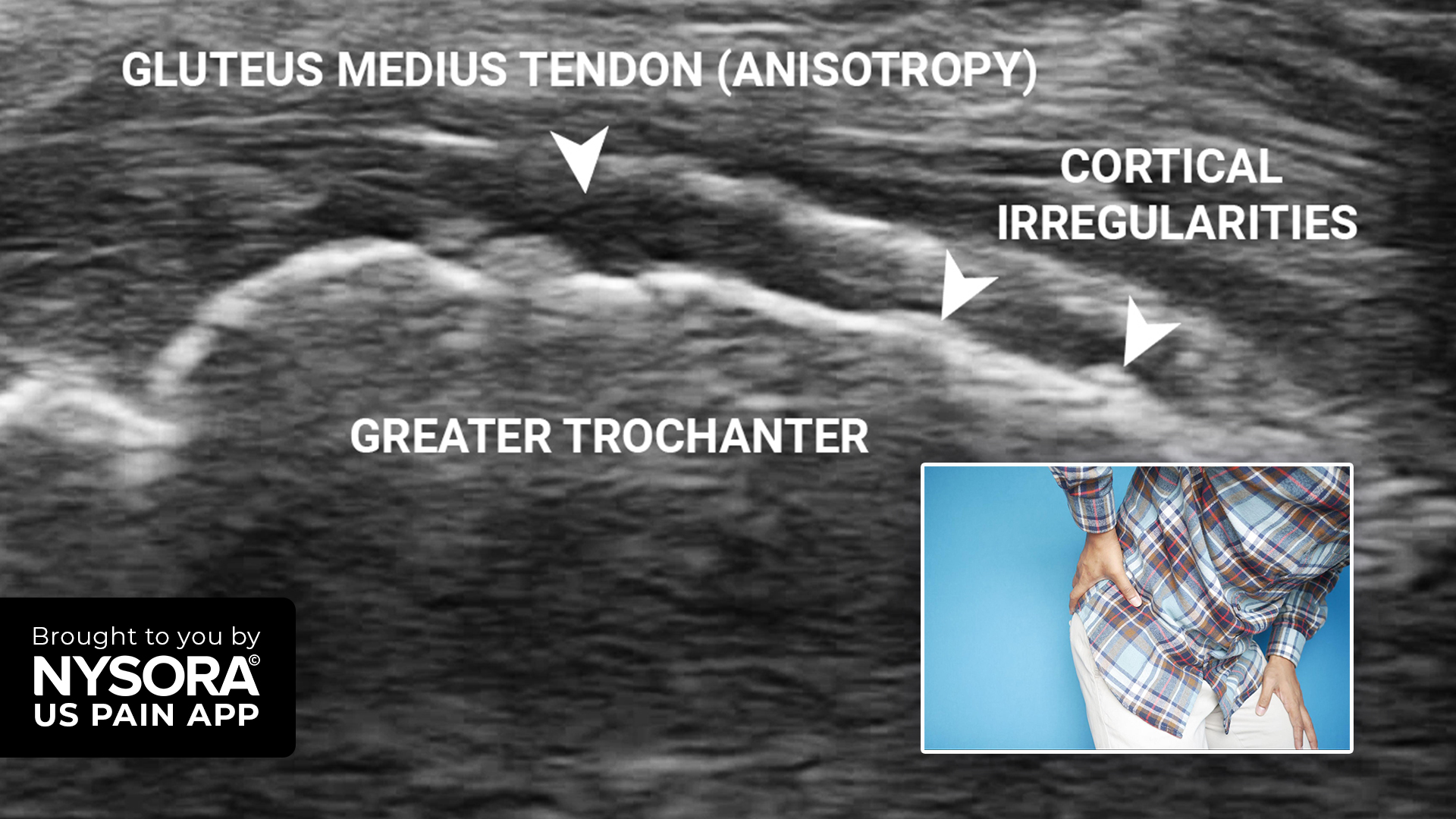
A 65-year-old man with diabetes has been suffering left lateral hip pain for six months. He reports no fever and has no history of injury or previous interventions. The patient mentions that the pain intensifies during the night, making it difficult for him to sleep on that side. Moreover, non-steroidal anti-inflammatory drugs (NSAIDs) have been ineffective in alleviating his symptoms. Physical examination Left lateral hip pain No back pain No radiation or referral of pain No aggravating or relieving factors Hot fomentation provides relief Ultrasound findings MSK ultrasound of the left hip Anisotropic gluteus medius tendon Cortical irregularities on the greater trochanter at the insertion site of the gluteus medius tendon Diagnosis The patient was diagnosed with greater trochanteric pain syndrome (GTPS) caused by gluteus medius tendinopathy. Previously referred to as trochanteric bursitis, GTPS arises from degenerative alterations in the gluteal tendons and bursa. This condition results in pain along the outer thigh, which is aggravated by activities such as sitting, climbing stairs, engaging in high-impact sports, or lying on the affected side. Discover more about the treatment strategy, patient outcome, and other unique case studies in the US Pain App. Ready to expand your knowledge? Click HERE and get the ultimate app for chronic pain procedures.
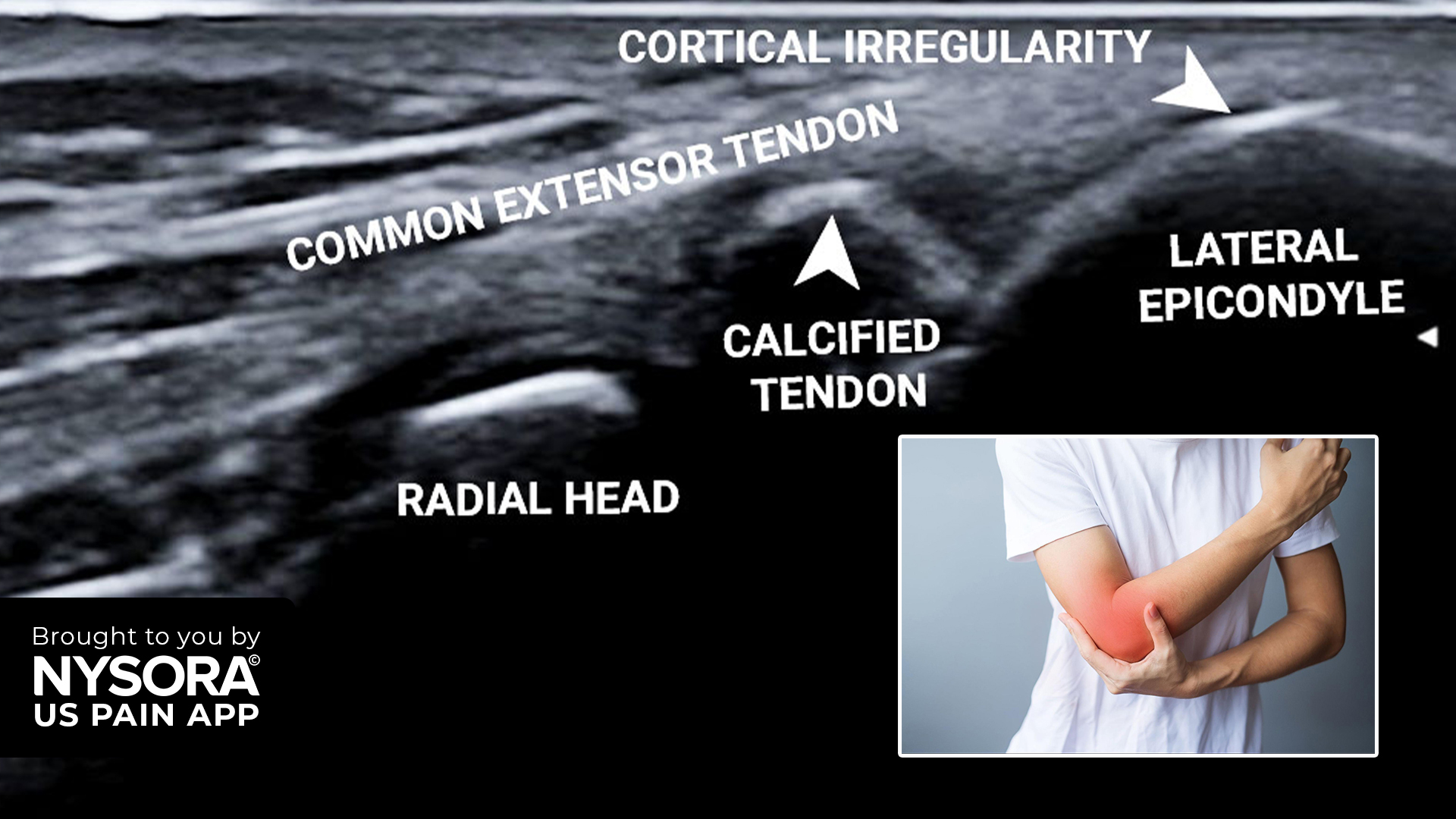
Lateral epicondylitis, commonly known as tennis elbow, is a prevalent condition characterized by pain and tenderness around the lateral aspect of the elbow. The condition predominantly affects individuals engaged in repetitive upper extremity motions, such as athletes and professionals involved in repetitive hand movements. In this article, we delve into a case study of a 30-year-old woman diagnosed with lateral epicondylitis and explore the diagnostic procedures and treatment strategies. Case presentation Patient background: Age/Gender: 30-year-old woman Occupation: Ultrasound application specialist Symptoms: Persistent lateral elbow pain in the left upper limb for 4 years, exacerbated by wrist extension. Previous treatments: Rest, splints, analgesics, and a steroid injection without significant relief. The patient reported severe local tenderness over the lateral epicondyle, suggestive of lateral epicondylitis, a condition often associated with overuse or repetitive stress injuries. Diagnosis Physical examination Observation: No localized redness or swelling. Palpation: Tenderness over the lateral epicondyle. Testing: Cozen’s test was positive. Ultrasound findings Tendon heterogeneity: Indicative of epicondylalgia or epicondylopathy. Cortical irregularities: Seen over the lateral epicondyle. Calcification: Within the common extensor tendon. Neoangiogenesis: Detected on color Doppler, indicating acute inflammation at the tendon attachment. Imaging tips: Echogenicity: Always assess the tendon’s echogenicity; heterogeneity is pathognomonic for epicondylitis. Multiple views: Utilize different transducer positions and views (long-axis and short-axis) to demonstrate all pathological signs. Laboratory Tests Fasting blood sugar: 86 mg/dL Erythrocyte sedimentation rate (ESR): 8 mm/h Diagnostic summary: Primary Diagnosis: Lateral epicondylitis (epicondylalgia, epicondylopathy). Differential diagnosis: Posterior interosseous nerve entrapment, lateral collateral ligament tear. Treatment approach: Platelet-rich plasma (PRP) injection Injection technique PRP Injection Overview: Objective: Regenerative therapy for the common extensor tendon and subsequent pain relief. Anatomy involved: The extensor carpi radialis brevis (ECRB) is the most commonly involved tendon. Other tendons like the extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris may also be […]
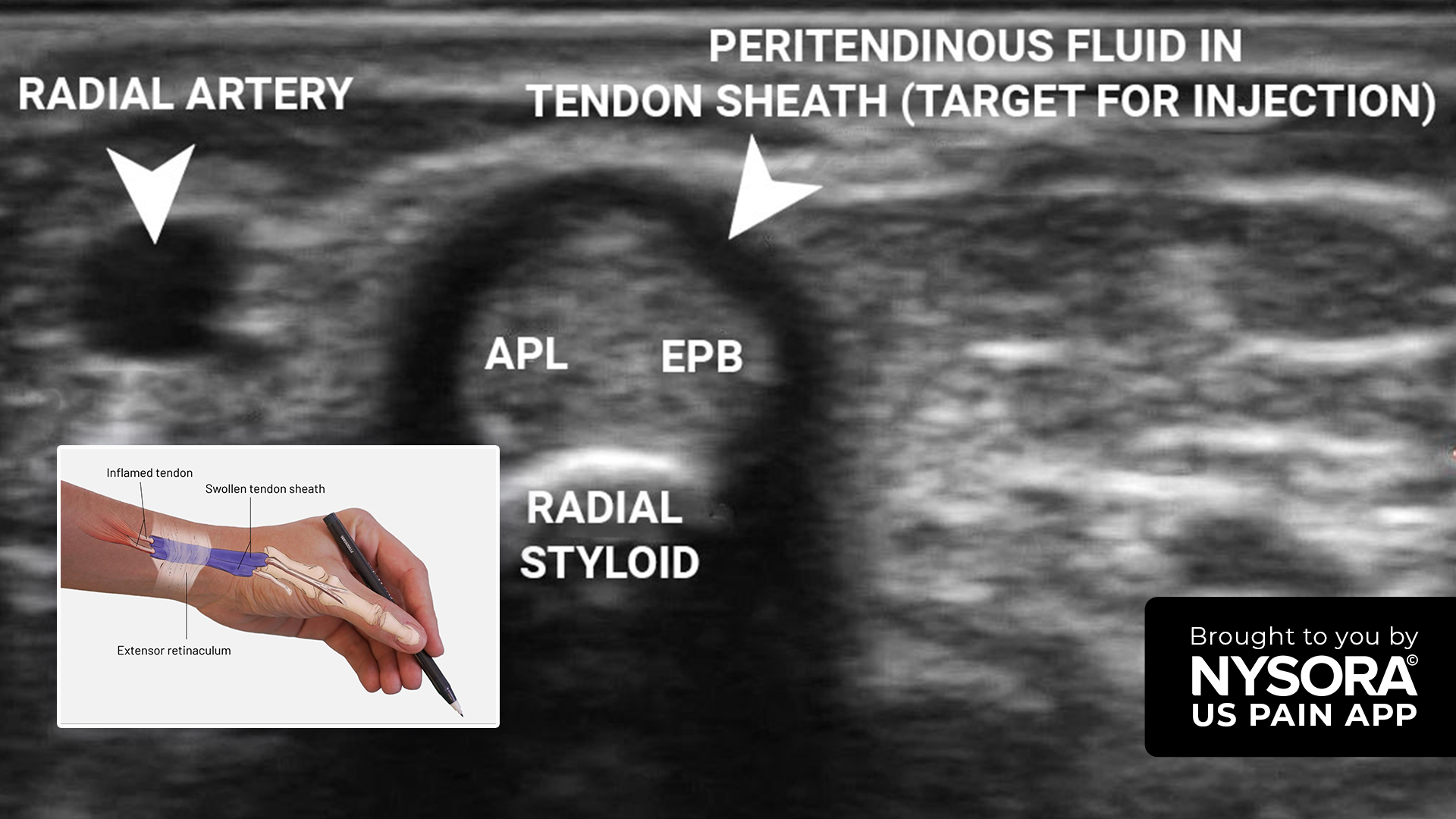
De Quervain’s tenosynovitis is a painful condition affecting the tendons on the thumb side of the wrist. It is particularly prevalent among individuals engaged in repetitive hand movements, such as those working in manual labor or with frequent use of the hands. This article presents a detailed case study of a 56-year-old woman diagnosed with De Quervain’s tenosynovitis. Case presentation Patient background: Age/gender: 56-year-old woman Occupation: Worked in a printing press for 6 years Symptoms: Chronic pain in the left hand for six months History: No history of hand injury The patient presented with chronic pain localized to the radial aspect of the wrist, which had progressively worsened over the past six months. Her occupational history involving repetitive hand movements suggested a potential overuse injury. Diagnosis Physical examination Finkelstein’s test: Positive. Ultrasound Findings Transverse View: Shows a thin rim of inflammatory fluid surrounding the tendons in extensor compartment 1. Longitudinal View: Reveals swollen tendons (abductor pollicis longus [APL] and extensor pollicis brevis [EPB]) with surrounding inflammatory fluid. Imaging Summary: Diagnosis: De Quervain’s tenosynovitis. Ultrasound role: Provides detailed imaging of the inflamed tendons and surrounding structures, allowing for precise diagnosis and treatment planning. Treatment Corticosteroid injection overview: Objective: Pain relief and reduction of inflammation in the affected tendons. Target area: Extensor compartment 1 tendon sheath over the wrist. Ultrasound-guided injection technique: Ultrasound setup: Transducer: 3-13 MHz linear transducer, preferably a hockey stick probe for better needle visualization. Preset: Musculoskeletal. Orientation: Axial. Depth: 1 cm. Patient positioning: Position: Patient supine with wrist in a semi-pronated position. A gel tube is placed under the wrist to achieve minimal ulnar deviation for better imaging. Landmarks identification: Key landmarks: APL, EPB tendons, and surrounding inflammatory fluid. Needle insertion: Sterile preparation: Sterilize the wrist, hand, and transducer. Local anesthetic: Infiltrate with 0.5 mL of 2% lidocaine […]

A 45-year-old female patient came in reporting chronic left shoulder pain lasting for three months after a minor injury. The pain primarily centered around the upper arm and the supraspinous fossa, worsening notably at night. Additionally, incidental pain was present on shoulder abduction. Physical examination Painful arc present Neer’s test: Positive Hawkins-Kennedy test: Positive Ultrasound findings Supraspinatus tendon at the level of the superior facet of the greater tuberosity: Normal Long-axis view of the rotator cuff at the level of the superior facet of the greater tuberosity. Supraspinatus tendon at the level of the inferior facet of the greater tuberosity: Minimal bursal surface tear, intrasubstance tears Long-axis view of the rotator cuff at the level of the inferior facet of the greater tuberosity. Short-axis view of the supraspinatus tendon: Normal Short-axis view of the rotator cuff. Diagnosis The patient was diagnosed with subacromial impingement syndrome secondary to rotator cuff tendinopathy. Subacromial impingement syndrome results from compression, irritation, or inflammation of the rotator cuff tendons in the subacromial space. It causes shoulder pain, weakness, and limited shoulder mobility, often due to factors like repetitive overhead activities or structural issues. This narrowing of the subacromial space compresses the rotator cuff tendons and subacromial bursa. In this particular case, the impingement was attributed to rotator cuff tendinopathy. Read more about the treatment, patient outcome, and other case studies in the US Pain App. Ready to elevate your knowledge? Tap HERE to download the go-to app for chronic pain procedures.
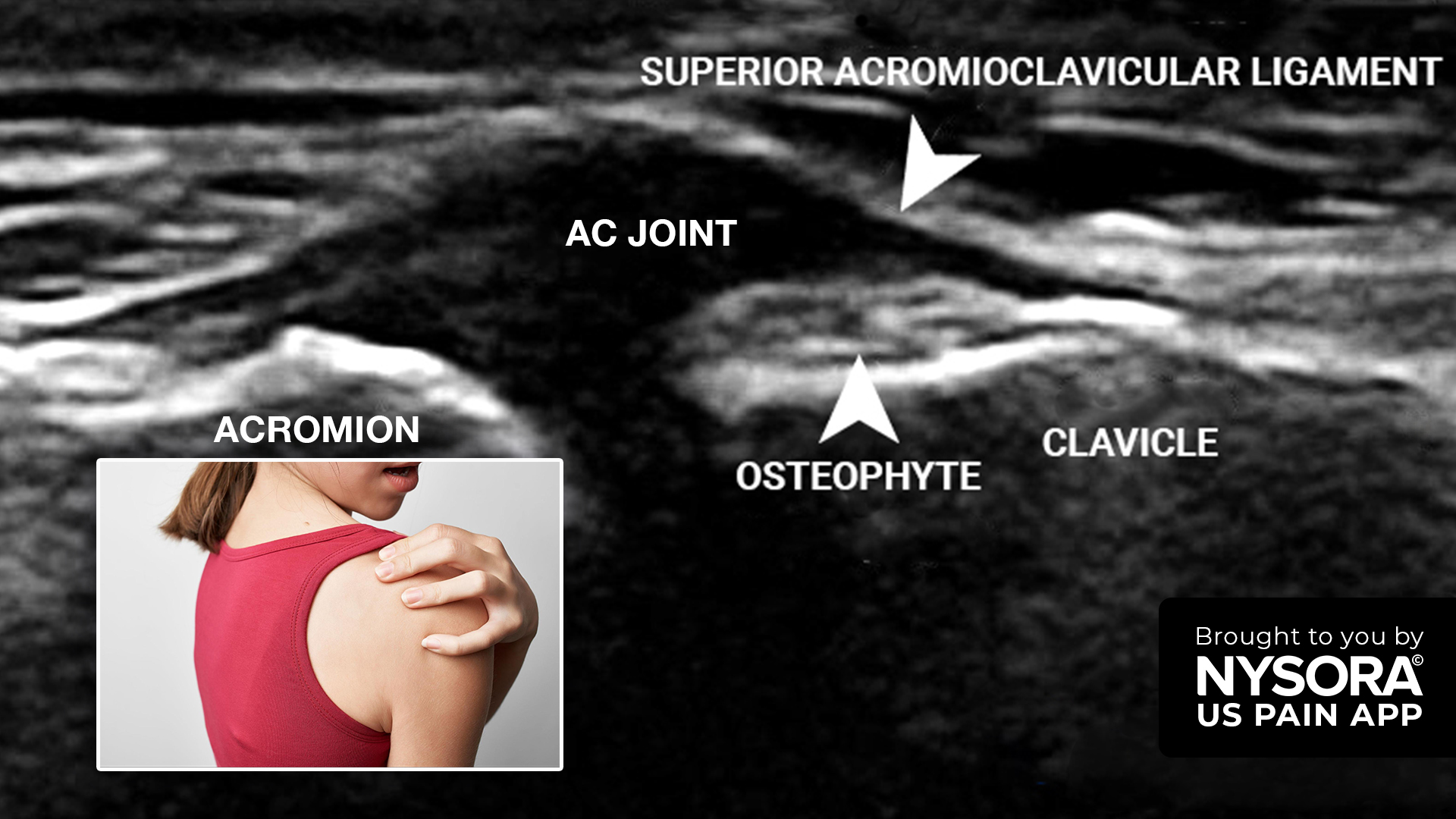
Acromioclavicular (AC) joint arthritis is a common cause of shoulder pain, particularly among individuals who engage in repetitive manual activities. In this article, we will discuss the case of a 65-year-old woman with AC joint arthritis and the use of ultrasound-guided injection as an effective treatment option for pain relief. Case presentation A 65-year-old female manual laborer presented with a 4-month history of left shoulder pain. Her symptoms included: Pain over the anteromedial region of the shoulder. Pain on external rotation. Superior shoulder pain, especially at night. This type of presentation is typical of AC joint arthritis, especially in individuals whose work or lifestyle places frequent stress on their shoulders. Diagnosis Physical examination Painful arc Scarf test: Positive O’Brien’s test: Positive Imaging and laboratory findings Ultrasound: An ultrasound of the AC joint showed space narrowing, capsular distension, and the presence of an osteophyte, all consistent with AC joint arthritis. Transverse view of the AC joint space showing space narrowing, capsular distension, and an osteophyte. X-ray: X-ray imaging revealed rotator cuff arthropathy and AC joint arthritis, with joint space reduction. X-ray image of the left shoulder. Fasting blood sugar: The patient’s fasting blood sugar was 102 mg/dL, within the normal range, ruling out diabetic complications as a cause of the pain. Final diagnosis The patient was diagnosed with acromioclavicular joint arthritis and supraspinatus tendinopathy. AC joint arthritis arises from the deterioration of cartilage within the AC joint, often due to repetitive stress. Supraspinatus tendinopathy is commonly associated with impingement in the subacromial space, leading to inflammation and degeneration of the tendon. Treatment: Ultrasound-guided AC joint injection Given the severity of the patient’s pain and the failure of conservative treatment to provide adequate relief, an ultrasound-guided injection of the AC joint was chosen as the next step. This minimally invasive procedure involves […]
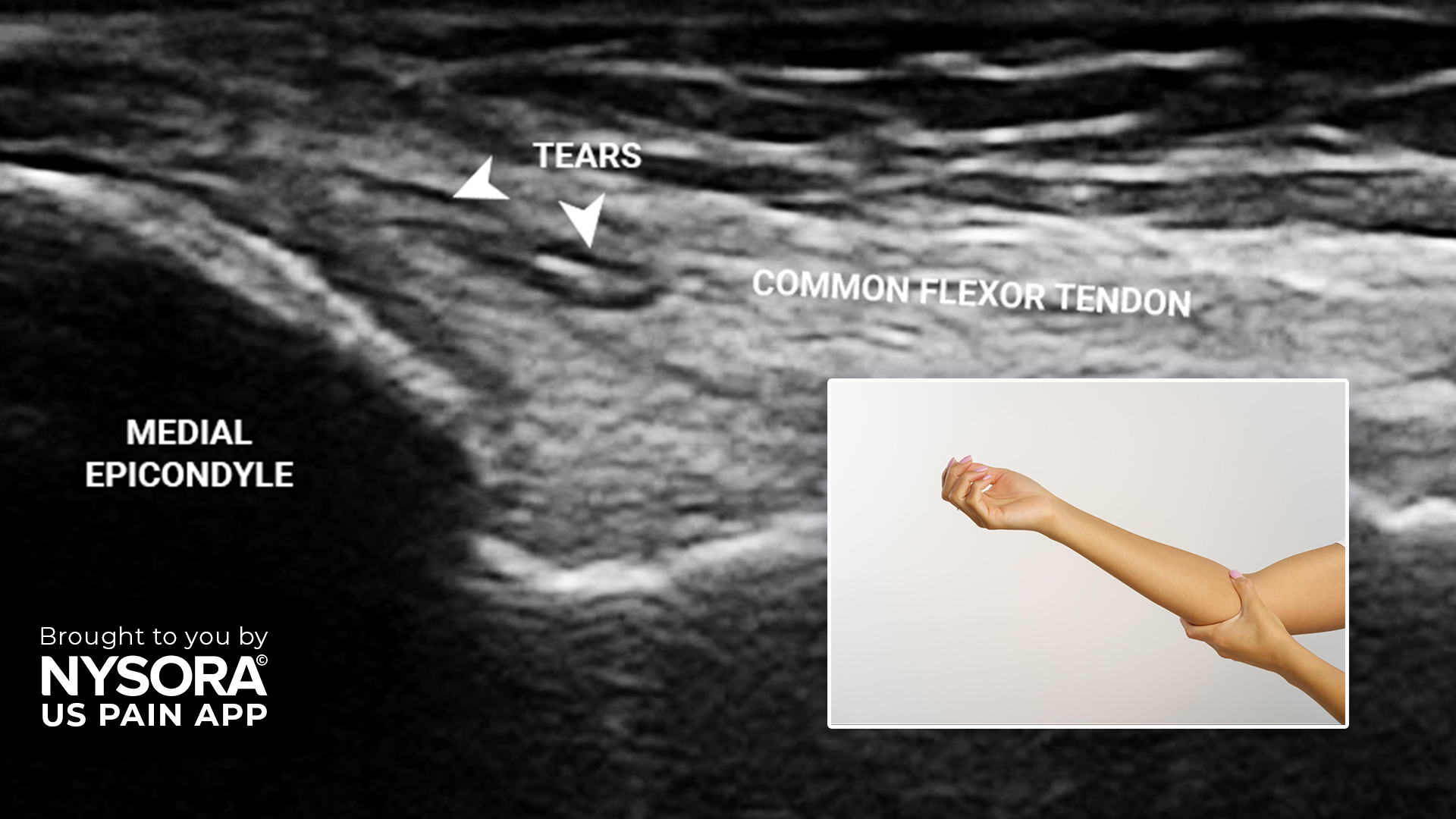
Medial epicondylitis, commonly known as golfer’s elbow, is a chronic condition characterized by pain and inflammation of the tendons that attach to the medial epicondyle of the elbow. This condition often results from repetitive wrist and forearm movements and can lead to significant discomfort and functional impairment. In this article, we present a case study of a 33-year-old woman diagnosed with golfer’s elbow. Case presentation Patient background: Age/gender: 33-year-old woman Symptoms: Right medial elbow pain persisting for one year following a minor trauma Previous treatment: Physical therapy and NSAIDs, with no significant improvement The patient reported ongoing pain in the medial aspect of her right elbow, which significantly affected her daily activities. Despite conservative management, including physical therapy and NSAIDs, her symptoms persisted. Diagnosis Physical examination Observation: No redness or edema noted. Palpation: Tenderness over the medial epicondyle. Polk’s test: Positive for medial epicondylitis. Laboratory parameters and imaging Fasting blood sugar: 100 mg% Erythrocyte sedimentation rate: 10 mm/hr Nerve conduction study: Normal Ultrasound findings: Tendon tears: Minimal tears in the common flexor tendon at the insertion point onto the medial epicondyle. Long axis view of the common flexor tendon and medial epicondyle. Note the tears at the insertion point. Joint effusion: Small effusion in the anterior joint recess of the elbow. Long axis view of the posterior elbow revealing a small effusion in the anterior joint recess. Imaging summary: Diagnosis: Medial epicondylitis. Differential diagnoses: Pronator overuse syndrome, cubital tunnel syndrome, arthritis, cervical radiculopathy. Treatment: Steroid injection Steroid injection overview: Objective: Pain relief by reducing inflammation at the affected site. Injection site: Superficial to the common flexor tendon at its insertion onto the medial epicondyle. Alternative treatments: Options: Dry needling, dextrose prolotherapy, botox, and PRP injection. Patient choice: The patient opted for a steroid injection for quicker pain relief, although PRP […]
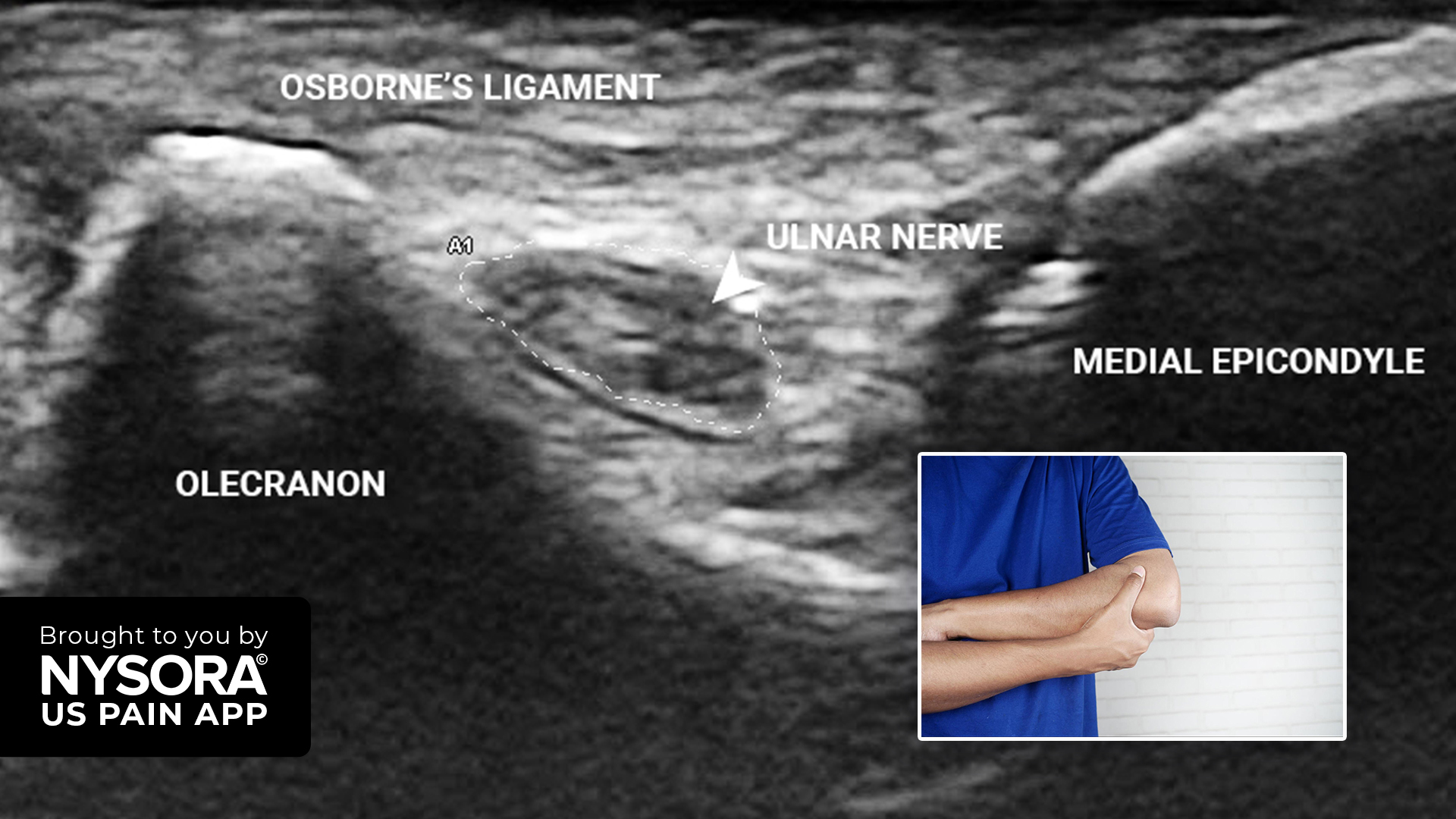
A 65-year-old orthopedic surgeon presents with pain along the ulnar aspect of the right forearm and hand, lasting for one year. The patient does not report any weakness in these areas and has no comorbidities. He previously underwent an ulnar nerve hydrodissection, a procedure to relieve pressure around the nerve, which reduced the pain by 80%. However, due to persistent occasional pain along the ulnar border of the forearm, he presented for further treatment. Physical examination Pain was not associated with any activity and there were no relieving factors No redness or wasting of the forearm No hypothenar wasting No evidence of ulnar claw hand Tinel sign: Positive Sensation: Light touch and 2-point discrimination were normal Froment’s sign: Negative Ultrasound findings MRI imaging revealed an ulnar nerve entrapment at the level of the medial epicondyle. The reference value for a swollen nerve is set at ≥ 10 mm2, according to the meta-analysis by Chang et al. (2018). Transverse view of the elbow in a neutral position at the level of the edial epicondyle. Here, the ulnar nerve measured 5.9 x 1.6 mm. UCL, ulnar collateral ligament. m Transverse view of the elbow in a flexed position at the level of the medial epicondyle. Here, the ulnar nerve measured 3.1 x 6.8 mm. Diagnosis The patient was diagnosed with cubital tunnel syndrome, which is caused by the compression of the ulnar nerve at the elbow. The ulnar nerve entrapment leads to numbness and pain in the forearm and specific fingers. It is the second most common neuropathy of the arm after carpal tunnel syndrome. Discover more about the treatment strategy, patient outcome, and other unique case studies in the US Pain App. Ready to expand your knowledge? Click HERE and get the ultimate app for chronic pain procedures.
Featuring tried-and-true US-guided Pain blocks techniques used by practitioners worldwide


Join our mailing list and get weekly educational updates delivered straight to your inbox.