Catherine Vandepitte, Ana M. Lopez, Sam Van Boxstael, and Hassanin Jalil
FACTS
- Indications: Distal foot and toe surgery
- Transducer position: about the ankle; depends on the nerve to be blocked
- Goal: local anesthetic spread surrounding each individual nerve
- Local anesthetic: 3–5 mL per nerve
GENERAL CONSIDERATIONS
Using an ultrasound (US)-guided technique affords a practitioner the ability to reduce the volume of local anesthetic required for ankle block. Because the nerves involved are located relatively close to the surface, ankle nerve blocks are easy to perform; however, knowledge of the anatomy of the ankle is essential to ensure success.
ULTRASOUND ANATOMY
Ankle nerve block involves anesthetizing five separate nerves: two deep and three superficial nerves. The two deep nerves are the tibial nerve and the deep peroneal nerve, and the three superficial nerves are the superficial peroneal, sural, and saphenous nerves. All nerves, except the saphenous, are terminal branches of the sciatic nerve; the saphenous nerve is a sensory branch of the femoral nerve.
Tibial Nerve
The tibial nerve is the largest of the five nerves at the ankle level and provides innervation to the heel and sole of the foot. With the linear transducer placed transversely at (or just proximal to) the level of the medial malleolus, the nerve can be seen immediately posterior to the posterior tibial artery (Figures 1, 2, and 3). Color Doppler can be very useful in locating the posterior tibial artery when it is not readily apparent. The nerve typically appears hyperechoic with honeycomb pattern. A useful mnemonic for the relevant structures in the vicinity is Tom, Dick ANd Harry, which refers to, from anterior to posterior, the tibialis posterior tendon, flexor digitorum longus tendon, artery/nerve/vein, and flexor hallucis longus tendon. These tendons can resemble the nerve in appearance, which can be confusing. The nerve’s intimate relationship with the artery should be kept in mind to avoid misidentification. If in doubt, track the structure proximally: tendons will turn into muscle bellies, whereas the nerve will not change in appearance.
FIGURE 1. Transducer position and needle insertion for a nerve block of the tibial nerve using an in-plane technique.
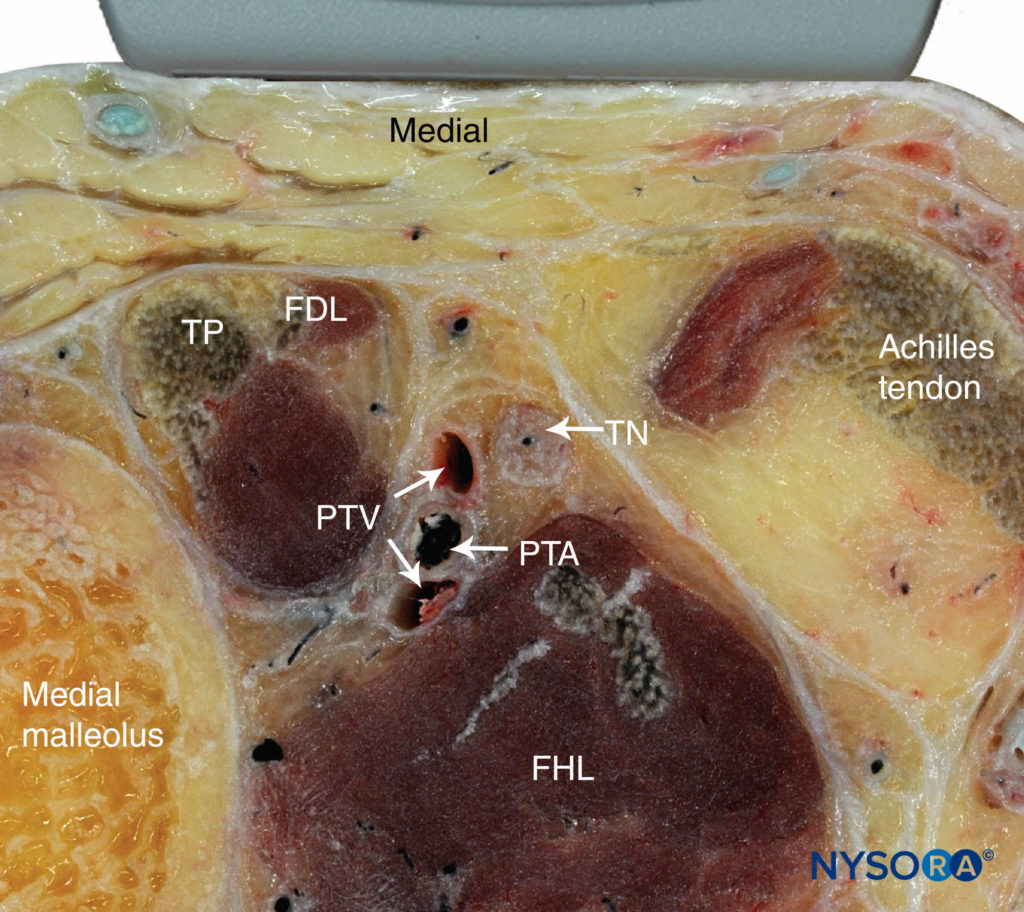
FIGURE 2. Cross-sectional anatomy of the tibial nerve at the level of the ankle. Shown are the posterior tibial artery (PTA) and vein (PTV) behind the medial malleolus , the tibialis posterior (TP) and the flexor digitorum longus (FDL). The tibial nerve (TN) is just posterior to the posterior tibial vessels and superficial to the flexor hallucis longus muscle (FHL). (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
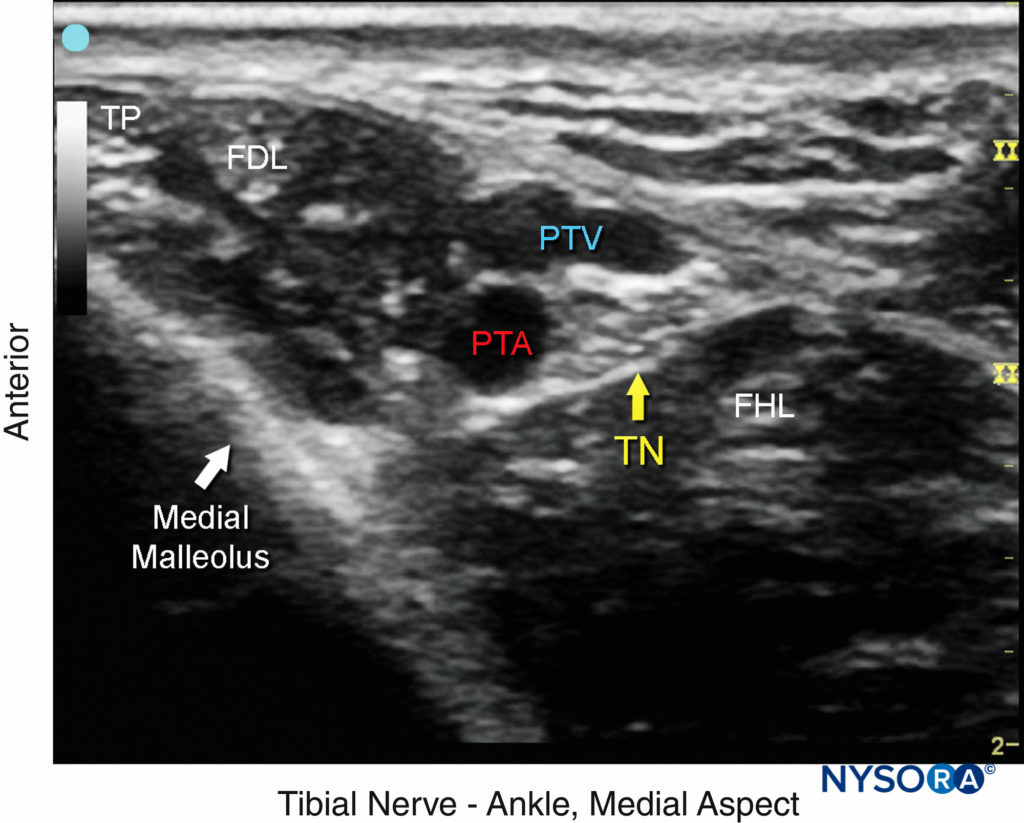
FIGURE 3. The tibial nerve (TN) is seen posterior and deep to the posterior tibial artery (PTA). TP, tibialis posterior; FDL, flexor digitorum longus; FHL, flexor hallucis longus; PTV, posterior tibial vein.
From the Compendium of Regional Anesthesia: Cognitive priming for a tibial nerve block at the level of the ankle.
Deep Peroneal Nerve
This branch of the common peroneal nerve innervates the ankle extensor muscles, the ankle joint and the web space between the first and second toes. As it approaches the ankle, the nerve crosses the anterior tibial artery from a medial to lateral position. A transducer placed in the transverse orientation at the level of the extensor retinaculum will show the nerve lying immediately lateral to the artery, on the surface of the tibia (Figures 4, 5, and 6). In some individuals the nerve courses along the medial side of the artery. The nerve usually appears hypoechoic with a hyperechoic rim, but it is small and often difficult to distinguish from the surrounding tissue.
FIGURE 4. Transducer position and needle insertion to nerve block the deep peroneal nerve at the level of the ankle.
(Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
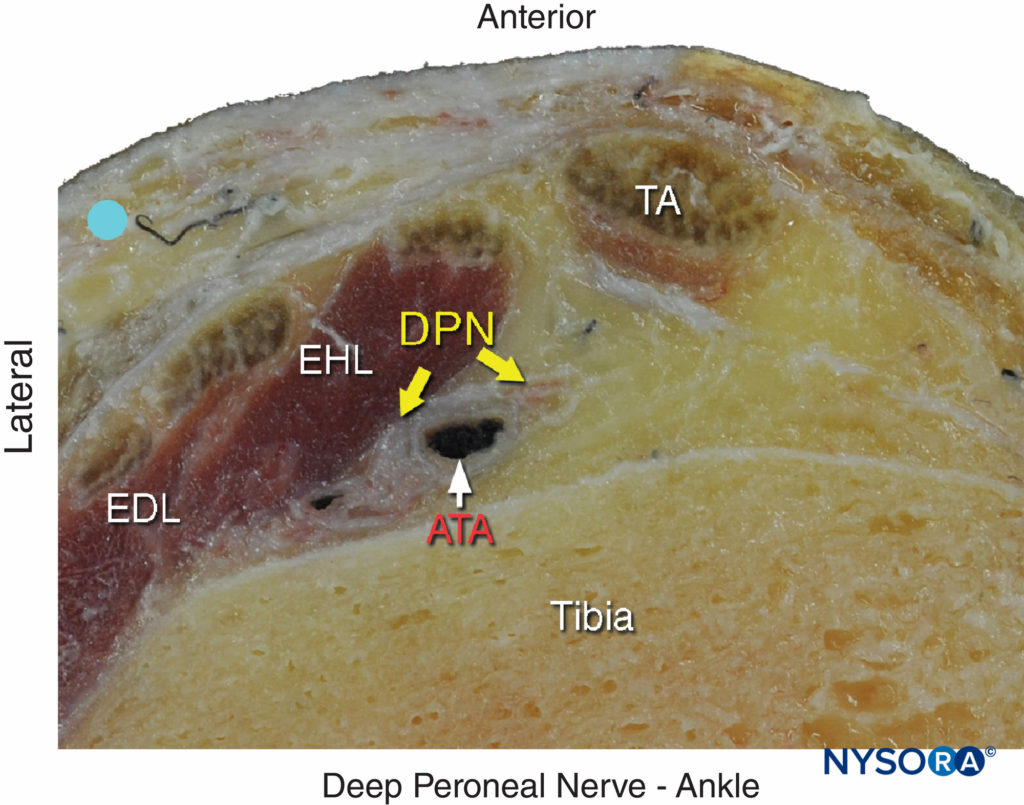
FIGURE 5. Cross-sectional anatomy of the deep peroneal nerve at the level of the ankle. The deep peroneal nerve (DPN) is located just lateral to anterior tibial artery (ATA) and between extensor hallucis longus (EHL) and tibia. Note the proximity of the extensor digitorum longus (EDL) and the tibialis anterior (TA), which can serve as an important landmark; to locate it, flex and extend the patient’s great toe manually. The deep peroneal nerve appears divided in this section. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York:McGraw-Hill, 2011.)
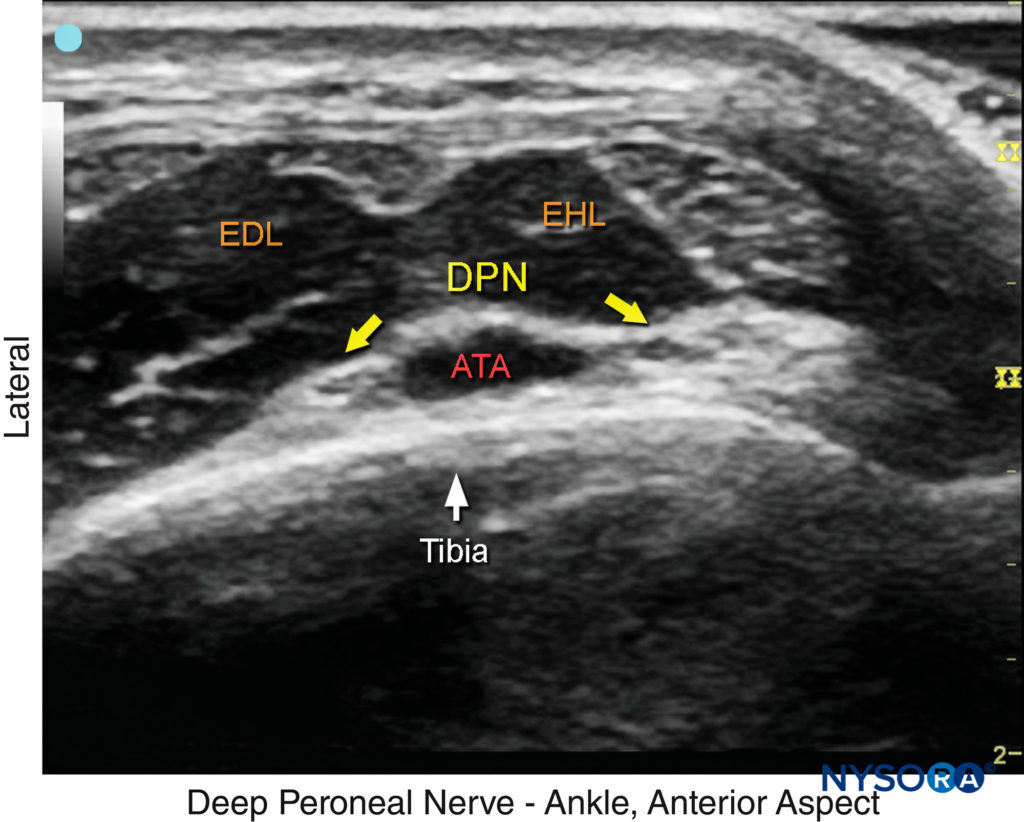
FIGURE 6. US image of the deep peroneal nerve (DPN), seen at the surface of the tibia just lateral to the anterior tibial artery (ATA). The nerve is divided in this image. The surrounding tendons are the extensor hallucis longus (EHL) and the extensor digitorum longus (EDL). (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
From the Compendium of Regional Anesthesia: Cognitive priming for a deep peroneal nerve block at the level of the ankle.
NYSORA Tips
When the deep peroneal nerve is difficult to identify on US, an injection around the artery may help with visualization.
Superficial Peroneal Nerve
The superficial peroneal nerve innervates the dorsum of the foot. It emerges to lie superficial to the fascia 10–20 cm above the ankle joint on the anterolateral surface of the leg and divides into two or three small branches. A transducer placed transversely on the leg, approximately 5-10 cm proximal and anterior to the lateral malleolus, will identify the hyperechoic nerve branches lying in the subcutaneous tissue immediately superficial to the fascia (Figures 7, 8, and 9). To identify the nerve proximal to its division, the transducer can be traced proximally until, at the lateral aspect, the extensor digitorum longus and peroneus brevis muscle can be seen with a prominent groove between them leading to the fibula (Figure 10).
FIGURE 7. Transducer position and needle insertion to nerve block the superficial peroneal nerve.
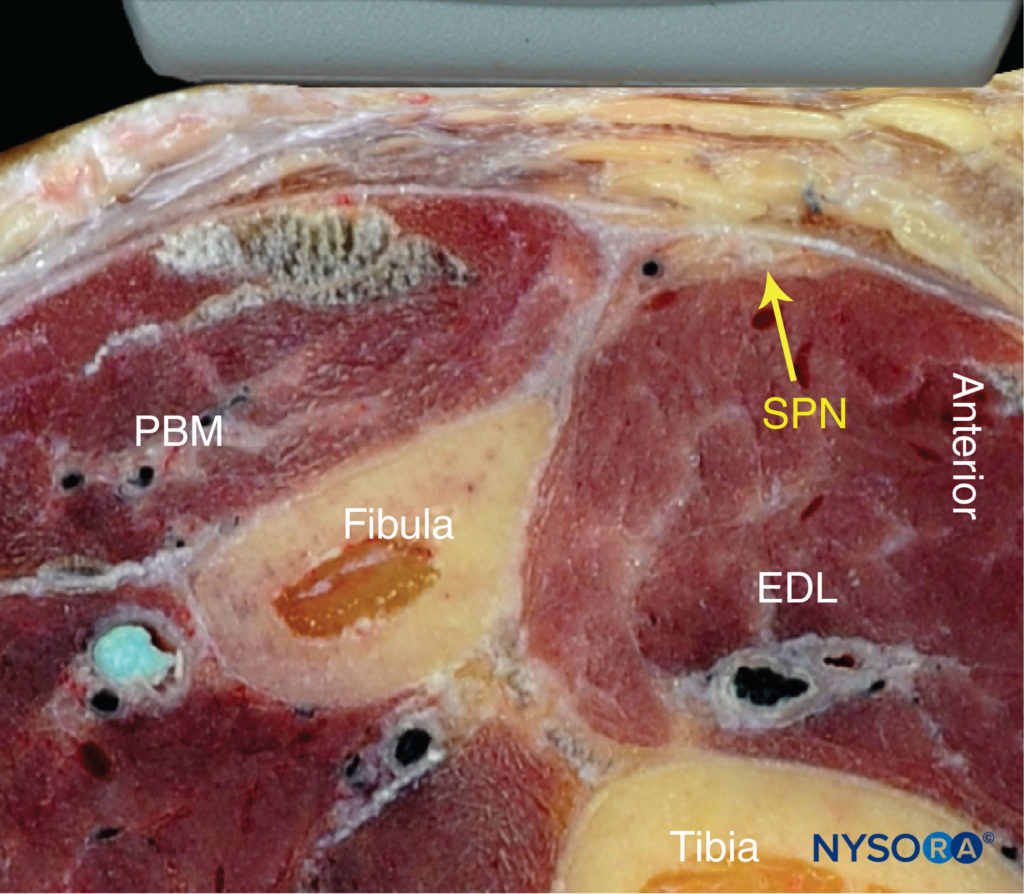
FIGURE 8. Cross-sectional anatomy of the superficial peroneal nerve (SPN). EDL, extensor digitorum longus muscle; PBM, peroneus brevis muscle. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound- Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
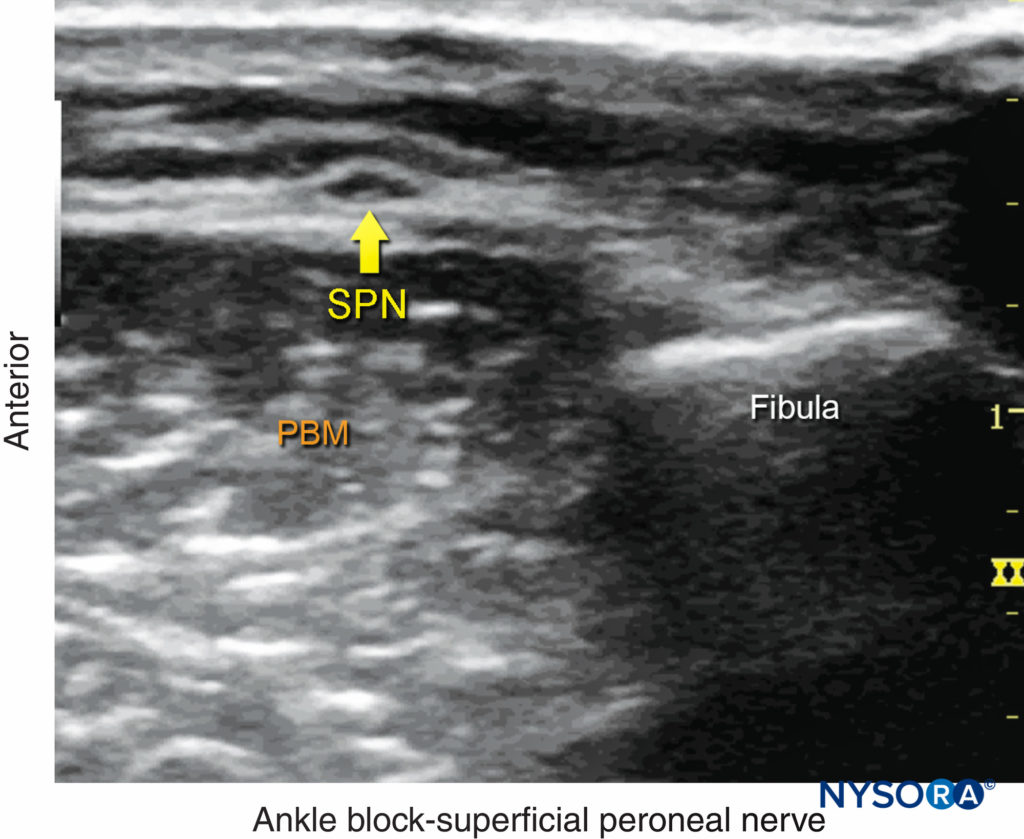
FIGURE 9. US anatomy of the superficial peroneal nerve (SPN). PBM, peroneus brevis muscle. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
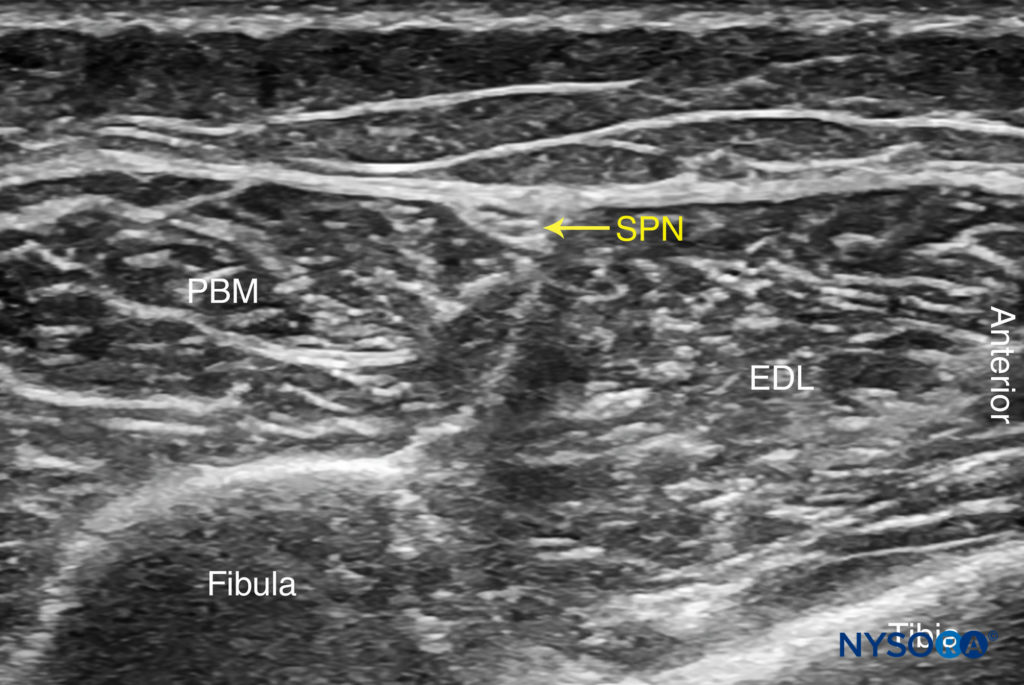
FIGURE 10. US anatomy of the superficial peroneal nerve with structures labeled. EDL, extensor digitorum longus muscle; PBM, peroneus brevis muscle; SPN, superficial peroneal nerve.
The superficial peroneal nerve is located in this groove, just deep to the fascia. Once it has been identified at this more proximal location, the nerve can be traced distally to the ankle or it can be blocked at this level. Because the superficial nerves are rather small, their identification with US is not always possible.
From the Compendium of Regional Anesthesia: Cognitive priming for a superficial peroneal nerve block at the level of the ankle.
NYSORA Tips
The use of a small-gauge needle (25-gauge) is recommended to decrease patient discomfort as needle insertion in this area can be painful.
Sural Nerve
The sural nerve innervates the lateral margin of the foot and ankle. Proximal to the lateral malleolus, the sural nerve can be visualized as a small hyperechoic structure that is intimately associated with the small saphenous vein superficial to the deep fascia.
The sural nerve, can be traced back along the posterior aspect of the leg, running in the midline superficial to the Achilles tendon and gastrocnemius muscles (Figures 11, 12, and 13). A calf tourniquet can be used to increase the size of the vein and facilitate its imaging; the nerve is often found in the immediate vicinity of the vein.
FIGURE 11. Transducer position and needle insertion to nerve block the sural nerve. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
FIGURE 12. Cross-sectional anatomy of the sural nerve at the level of the ankle. Shown is the sural nerve (SuN) in the immediate vicinity of the small saphenous vein (SSV). (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
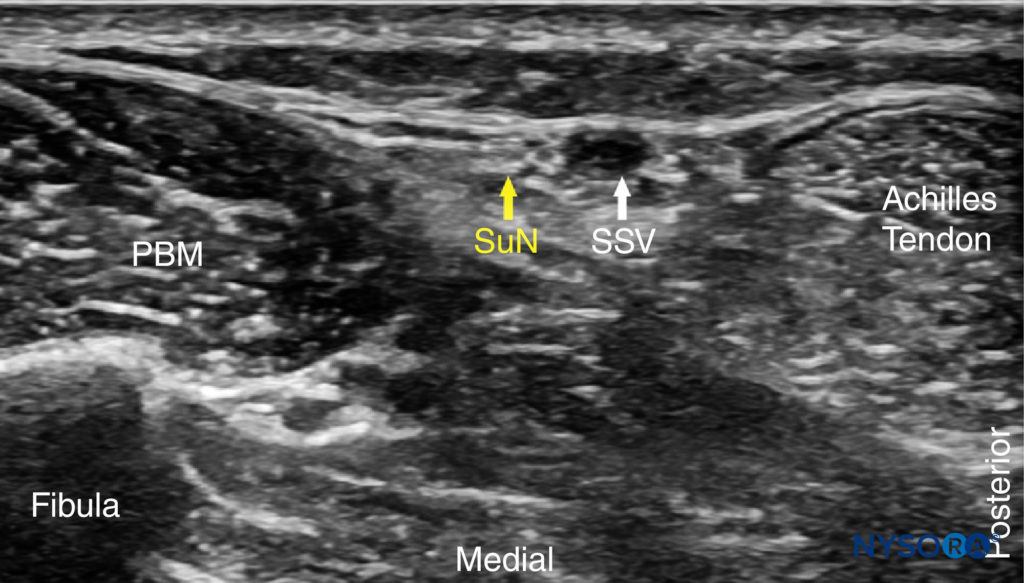
FIGURE 13. US anatomy of the sural nerve (SuN). Shown are the peroneus brevis muscle (PBM) and small saphenous vein (SSV).
From the Compendium of Regional Anesthesia: Cognitive priming for a sural nerve block at the level of the ankle.
Saphenous Nerve
The saphenous nerve innervates the medial malleolus and a variable portion of the medial aspect of the leg below the knee. The nerve travels down the medial leg alongside the great saphenous vein. Because it is a small nerve, it is best visualized 10–15 cm proximal to the medial malleolus, using the great saphenous vein as a landmark (Figures 14, 15, and 16). A proximal calf tourniquet can be used to assist in increasing the size of the vein.
FIGURE 14. Transducer position and needle insertion to nerve block the saphenous nerve. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
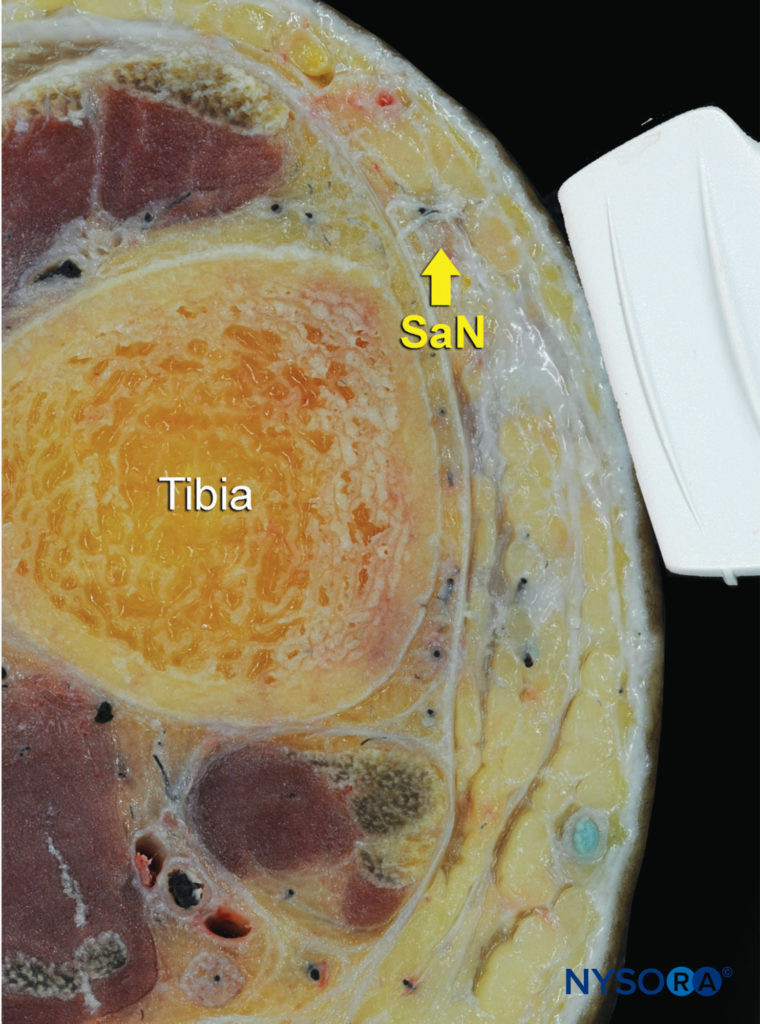
FIGURE 15. Cross-sectional anatomy of the saphenous nerve (SaN) at the level of the ankle. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
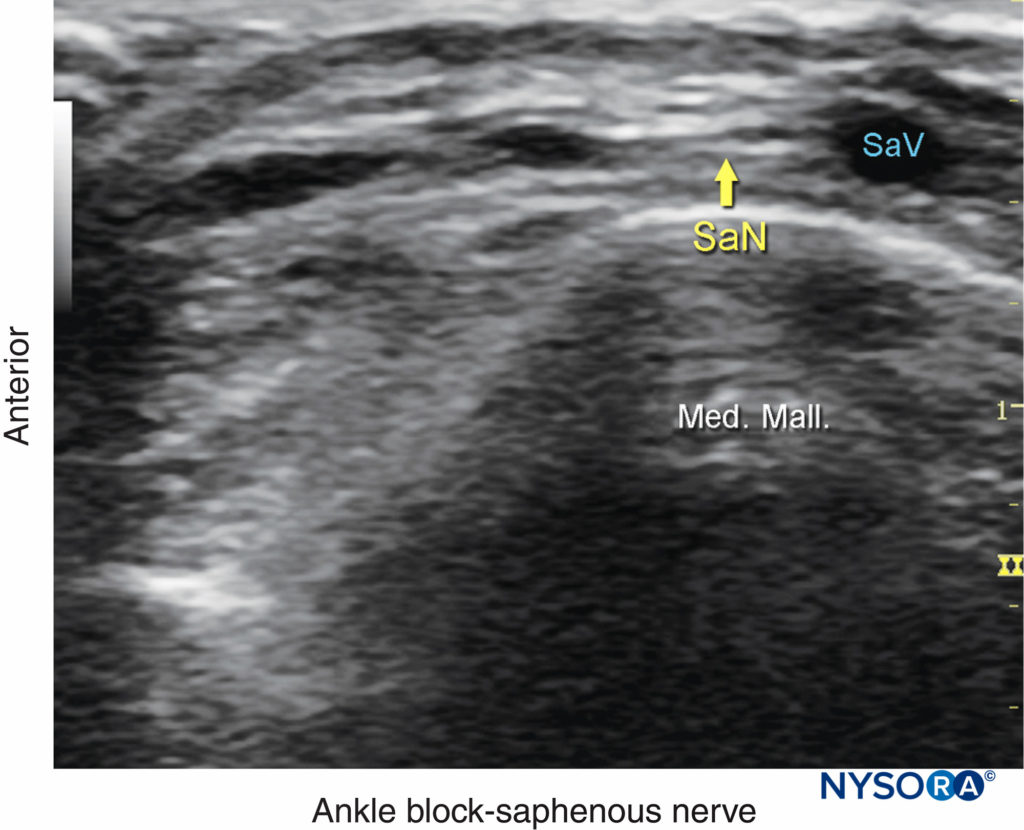
FIGURE 16. US anatomy of the saphenous nerve (SaN). Shown are the great saphenous vein (SaV) and the medial malleolus (Med. Mall.). (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
The nerve appears as a small hyperechoic structure, next to the vein. At this level the nerve often has several branches.
From the Compendium of Regional Anesthesia: Cognitive priming for a saphenous nerve block at the level of the ankle.
NYSORA Tips
When using veins as landmarks, use as little pressure as possible on the transducer in order to permit the veins to fill.
For a more comprehensive review of the distribution of each nerve, see Functional Regional Anesthesia Anatomy.
DISTRIBUTION OF ANESTHESIA
An ankle nerve block results in anesthesia of the entire foot.
EQUIPMENT
The equipment recommended for an ankle nerve block is:
- Ultrasound machine with linear transducer (8–18 MHz), sterile sleeve, and gel
- Standard nerve block tray
- Three 10-mL syringes containing local anesthetic
- A 1.5-inch, 22- to 25-gauge needle with low-volume extension tubing
- Sterile gloves
Learn more about Equipment for Peripheral Nerve Blocks
LANDMARKS AND PATIENT POSITIONING
This nerve block is usually performed with the patient in the supine position with a footrest underneath the calf to facilitate access to the ankle, especially for the tibial and sural nerve blocks. An assistant is helpful to maintain internal or external rotation of the leg as needed.
GOAL
The goal is to place the needle tip immediately adjacent to each of the five nerves and deposit local anesthetic until the spread around each nerve is accomplished.
TECHNIQUE
With the patient in the proper position, the skin is disinfected. For each of the nerve blocks, the needle can be inserted either in-plane or out-of-plane. Ergonomics often dictate which approach is most effective.
A successful nerve block is predicted by the spread of local anesthetic immediately adjacent to the nerve. Redirection to achieve circumferential spread is not necessary because these nerves are small, and the local anesthetic diffuses quickly into the neural tissue. A 3–5 mL of local anesthetic per nerve is typically sufficient for an effective nerve block.
TIPS
-
- If the smaller superficial nerves (sural, saphenous and superficial peroneal) are not seen, these nerves can be blocked simply by injecting local anesthetic into the subcutaneous tissue as a “skin wheal”; for the sural nerve, inject from the Achilles tendon to the lateral malleolus; for the superficial peroneal and the saphenous, inject anteriorly from one malleolus to the other, taking care to avoid injuring the great saphenous vein.
- The saphenous nerve block can be omitted in surgery on the forefoot and toes. In 97% of patients, the saphenous nerve innervation does not extend beyond the midfoot. However, an anatomical study found branches of the saphenous nerve reaching the first metatarsal in 28% of specimens.
REFERENCES
- Chin KJ, Wong NW, Macfarlane AJ, Chan VW: Ultrasound-guided versus anatomic landmark-guided ankle nerve blocks: a 6-year retrospective review. Reg Anesth Pain Med 2011;36:611–618.
- López AM, Sala-Blanch X, Magaldi M, Poggio D, Asuncion J, Franco CD: Ultrasound-guided ankle nerve block for forefoot surgery: the contribution of the saphenous nerve. Reg Anesth Pain Med 2012;37:554–557.
- Marsland D, Dray A, Little NJ, Solan MC: The saphenous nerve in foot
and ankle surgery: its variable anatomy and relevance. Foot Ankle Surg 2013;19:76–79. - Antonakakis JG, Scalzo DC, Jorgenson AS, et al: Ultrasound does not improve the success rate of a deep peroneal nerve block at the ankle. Reg Anesth Pain Med 2010;35:217–221.
- Benzon HT, Sekhadia M, Benzon HA, et al: Ultrasound-assisted and evoked motor response stimulation of the deep peroneal nerve. Anesth Analg 2009;109:2022–2024.
- Canella C, Demondion X, Guillin R, et al: Anatomic study of the superficial peroneal nerve using sonography. AJR Am J Roentgenol 2009;193: 174–179.
- Prakash, Bhardwaj AK, Singh DK, Rajini T, Jayanthi V, Singh G: Anatomic variations of superficial peroneal nerve: clinical implications of a cadaver study. Ital J Anat Embryol 2010;115:223–228.
- Redborg KE, Antonakakis JG, Beach ML, Chinn CD, Sites BD: Ultrasound improves the success rate of a tibial nerve block at the ankle. Reg Anesth Pain Med 2009;34:256–260.
- Redborg KE, Sites BD, Chinn CD, et al: Ultrasound improves the success rate of a sural nerve block at the ankle. Reg Anesth Pain Med 2009;34: 24–28.
- Russell DF, Pillai A, Kumar CS: Safety and efficacy of forefoot surgery under ankle nerve block anaesthesia. Scott Med J 2014;59:103–107.
- Snaith R, Dolan J: Ultrasound-guided superficial peroneal nerve block for foot surgery. AJR Am J Roentgenol 2010;194:W538.