Admir Hadzic, Ana M. Lopez, Catherine Vandepitte, and Xavier Sala-Blanch
FACTS
- Indications: Foot, ankle and Achilles tendon surgery
- Transducer position: Transverse over the popliteal fossa
- Goal: Local anesthetic spread surrounding the sciatic nerve within the epineural sheath
- Local anesthetic: 15–20 mL
GENERAL CONSIDERATIONS
The anatomy of the sciatic nerve in the popliteal fossa is variable, and the division into the tibial nerve (TN) and common peroneal nerve (CPN) occurs at an inconstant distance from the popliteal crease (Figure 1). With nerve stimulator–based techniques, larger volumes (eg, > 40 mL) of local anesthetic have been used to increase the chance of nerve block success.

FIGURE 1. Cross-sectional anatomy of the sciatic nerve in the popliteal fossa. Shown are the common peroneal nerve (CPN), tibial nerve (TN), popliteal artery (PA), popliteal vein (PV), femur, biceps femoris muscle (BFM), semimembranosus muscle (SmM), and semitendinosus (StM) muscle. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
However, US guidance reduces the volume required for a reliable nerve block because the injection can be halted once adequate spread is observed. The most common approaches to the popliteal sciatic nerve block are the lateral approach, with the patient in the supine or lateral position, and the posterior approach in the prone or lateral position (Figure 2). While the patient position and needle path differ between the two approaches, the rest of the technique details are similar.
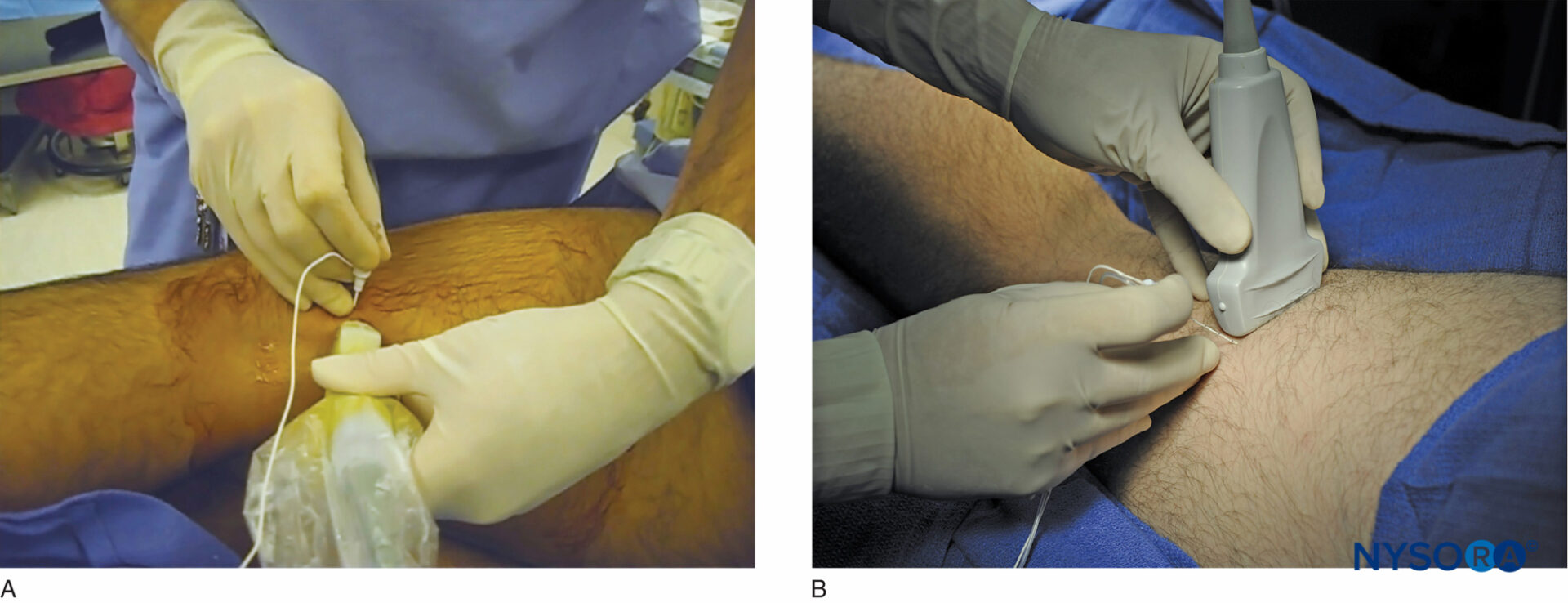
FIGURE 2. The posterior approach to the US-guided popliteal sciatic nerve block can be performed (A) with the patient in the lateral position, or (B) with the patient prone. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
The injection of local anesthetic must occur within the sciatic nerve sheath that contains both components of the nerve. The injection is ideally accomplished at the position where both components of the nerve are within the sheath but slightly separated by adipose tissue, allowing for safe placement of the needle between them. Although the sciatic nerve block can be accomplished with an injection around either nerve component, injecting into the space between both is more common in clinical practice.
ULTRASOUND ANATOMY
Beginning with the transducer in the transverse position at the popliteal crease, the popliteal artery is identified, aided with color Doppler US when necessary, at a depth of approximately 3–4 cm. The popliteal vein accompanies the artery at it is positioned just superficial (posterior) to it. On either side of the artery are the biceps femoris muscles (laterally) and the semimembranosus and semitendinosus muscles (medially). The tibial nerve is positioned superficial and lateral to the vein and is seen as a hyperechoic, oval or round structure with a honeycomb pattern (Figure 3). Asking the patient to dorsiflex and plantar flex the ankle makes the two sciatic nerve branches twist or move in relation to each other. Usually, tilting the transducer caudally is necessary to bring out the nerve from the neighboring adipose tissue.
 and the common peroneal nerve (CPN), are seen immediately lateral and superficial to the popliteal vein (PV) and artery (PA). This image was taken at 5 cm above the popliteal fossa crease, where the TN and CPN have just started diverging.")
FIGURE 3. Sonoanatomy of the sciatic nerve at the popliteal fossa. The two main divisions of the sciatic nerve, the tibial nerve (TN) and the common peroneal nerve (CPN), are seen immediately lateral and superficial to the popliteal vein (PV) and artery (PA). This image was taken at 5 cm above the popliteal fossa crease, where the TN and CPN have just started diverging.
Once the tibial nerve has been identified, the CPN is visualized slightly more superficial and lateral to the tibial nerve. The transducer should be slid proximally until the tibial and peroneal nerves are visualized coming together to form the sciatic nerve before its division (Figure 4). This junction usually occurs at a distance 5–10 cm from the popliteal crease but may occur very close to the crease or, less commonly, more proximally in the thigh.
 before its division. Shown are the ScN, superior and lateral to the popliteal artery (PA), positioned between the biceps femoris muscle (BFM) the semimembranosus muscle (SmM), and the semitendinosus muscle (StM).")
FIGURE 4 Sonoanatomy of the sciatic nerve (ScN) before its division. Shown are the ScN, superior and lateral to the popliteal artery (PA), positioned between the biceps femoris muscle (BFM) the semimembranosus muscle (SmM), and the semitendinosus muscle (StM).
As the transducer is moved proximally, the popliteal vessels move deeper and become more challenging to image. Adjustments in depth, gain, focus, and direction of the US beam should be made to keep the nerve visible at all times. At the popliteal fossa, the sciatic nerve typically is visualized at a depth of 2–4 cm.
NYSORA Tips
• Ultrasound imaging should specifically focus on identifying the sciatic nerve sheath (Vloka’s sheath) containing both components of the sciatic nerve (tibial and common peroneal nerves). Successful injection will deposit local anesthetic within the Vloka’s sheath
From the Compendium of Regional Anesthesia: Cognitive priming for a popliteal sciatic nerve block.
For a more comprehensive review of the sciatic nerve distribution, see Functional Regional Anesthesia Anatomy.
block DISTRIBUTION
Sciatic nerve block results in anesthesia of the lower limb below the knee, both motor and sensory, with the exception of the medial leg and foot, which is the territory of the saphenous nerve, a branch of the femoral nerve. The motor fibers to the hamstring muscles are spared; however, fibers to the posterior aspect of the knee joint are blocked (Figure 5).
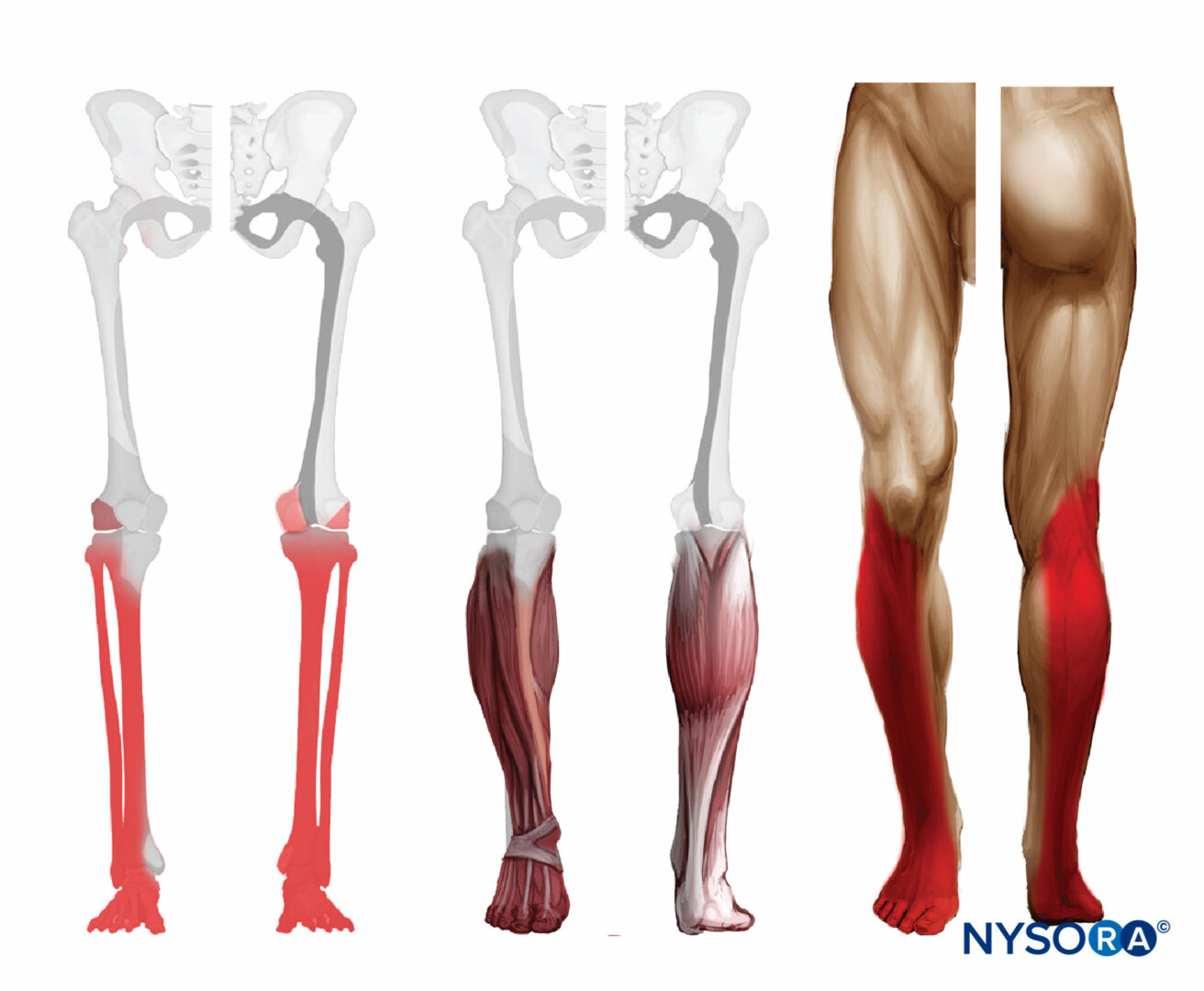
FIGURE 5. Expected distribution of the sciatic nerve sensory block at the level of the popliteal fossa.
EQUIPMENT
The equipment recommended for a popliteal sciatic nerve block includes the following:
- Ultrasound machine with a linear transducer (8–12 MHz), sterile sleeve, and gel
- Standard nerve block tray
- A 20-mL syringe containing local anesthetic
- 50- to 100-mm, 21- to 22-gauge, short-bevel, insulated stimulating needle
- Peripheral nerve stimulator
- Injection pressure monitor
- Sterile gloves
Learn more about Equipment for Peripheral Nerve Blocks
LANDMARKS AND PATIENT POSITIONING: LATERAL APPROACH
This nerve block is performed with the patient in the supine or lateral position. This can be accomplished either by resting the foot on an elevated footrest or flexing the knee while an assistant stabilizes the foot and ankle on the bed (Figure 6). If nerve stimulation is used, exposure of the calf and foot is required to observe motor responses.

FIGURE 6. Needle insertion technique to nerve block the sciatic nerve in the popliteal fossa using the lateral approach with the patient in the supine position. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
LANDMARKS AND PATIENT POSITIONING: POSTERIOR APPROACH
This nerve block is performed with the patient in the prone or lateral position (Figure 2). A small footrest is useful to facilitate identification of a motor response if nerve stimulation is used. A footrest also relaxes the hamstring tendons, making transducer placement and manipulation easier.
GOAL
The goal is to inject the local anesthetic within the common connective tissue (Vloka’s) sheath that envelops the TN and CPN. Alternatively, separate nerve blocks of TN and CPN can be performed.
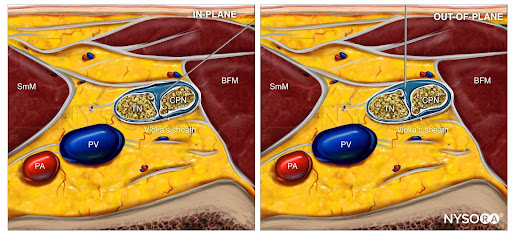
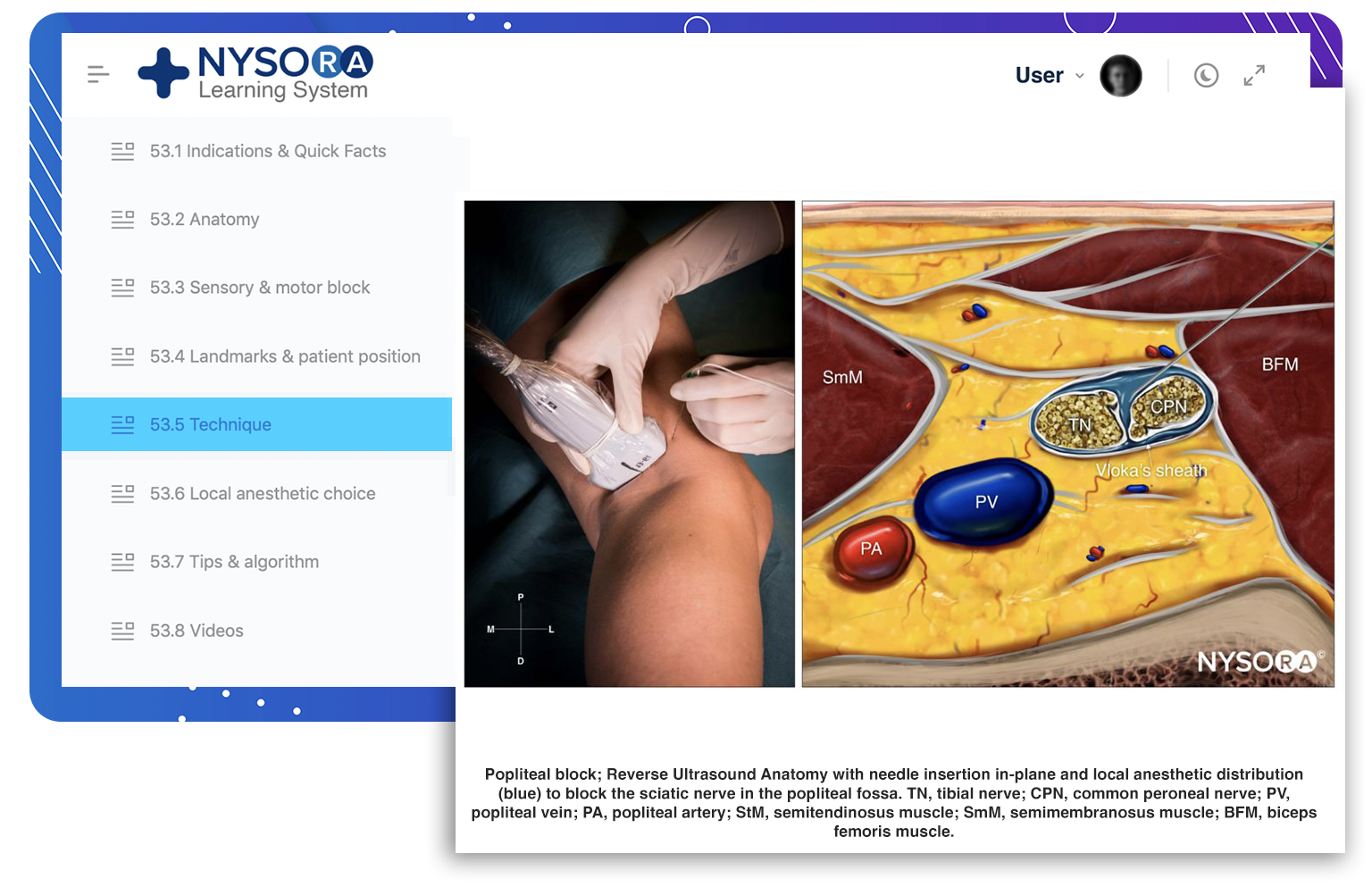
From the Compendium of Regional Anesthesia: Reverse Ultrasound Anatomy for a popliteal sciatic nerve block with needle insertion in-plane and out-of-plane and local anesthetic spread (blue). TN, tibial nerve; CPN, common peroneal nerve; PV, popliteal vein; PA, popliteal artery; SmM, semimembranosus muscle; BFM, biceps femoris muscle.
TECHNIQUE
The skin is disinfected and the transducer positioned to identify the sciatic nerve. If the nerve is not immediately apparent, tilting the transducer toward the feet can help improve the contrast and bring the nerve “out of the background”. Sliding the transducer slightly proximal or distal may improve the quality of the image and allow for better visualization.
It is recommended to perform the nerve block at the level where TN and CPN start diverging but are still in the common sciatic nerve (Vloka’s) sheath. For the lateral approach, a skin wheal is made on the lateral aspect of the thigh 2–3 cm above the lateral edge of the transducer, and the needle is inserted in plane in a horizontal orientation from the lateral aspect of the thigh and advanced toward the sciatic nerve (Figures 7 and 8).
 using the lateral approach. PA, popliteal artery.")
FIGURE 7. Simulated needle path and needle tip placement to nerve block the sciatic nerve (TN and CPN) using the lateral approach. PA, popliteal artery.
 in the popliteal fossa using the lateral approach. PA, popliteal artery.")
FIGURE 8. Simulated needle path and local anesthetic distribution to nerve block the sciatic nerve (TN and CPN) in the popliteal fossa using the lateral approach. PA, popliteal artery.
For the posterior approach, the needle is inserted in plane from lateral to medial (Figure 9) or out of plane (Figure 10). If nerve stimulation is used (0.5 mA, 0.1 msec), the contact of the needle tip with either branch of the nerve usually is associated with a motor response of the calf or foot. Once the needle tip is placed within the common sciatic nerve sheath, 1–2 mL of local anesthetic is injected to confirm the proper injection site. Such injection should result in a distribution of local anesthetic within the sheath, and separation of the TN and CPN within Vloka’s sheath (Figure 11).
 through the posterior approach, in plane from lateral to medial. PA, popliteal artery.")
FIGURE 9. Simulated needle path and needle tip placement to nerve block the sciatic nerve (TN and CPN) through the posterior approach, in plane from lateral to medial. PA, popliteal artery.
 through the posterior approach out of plane. PA, popliteal artery.")
FIGURE 10. Simulated needle path and proper needle tip placement to nerve block the sciatic nerve (TN and CPN) through the posterior approach out of plane. PA, popliteal artery.
 to nerve block the sciatic nerve (TN and CPN) through the posterior approach out of plane. PA, popliteal artery.")
FIGURE 11. Simulated needle path, needle tip position and local anesthetic spread (blue-shaded area) to nerve block the sciatic nerve (TN and CPN) through the posterior approach out of plane. PA, popliteal artery.
When local anesthetic injection does not appear to result in a spread inside the sciatic nerve sheath and around the sciatic nerve components, additional needle repositions and injections may be necessary. Correct injection is recognized when local anesthetic spreads proximally and distally to the site of the injection around both divisions of the nerve, which can be documented by observing the spread of the local anesthetic within Vloka’s sheath proximal to the site of injection. A single injection of local anesthetic typically suffices.
Supplementary video related to this nerve block can be found at Ultrasound-Guided Popliteal Sciatic Nerve Block Video
TIPS
- To improve needle visualization, a skin puncture site 2–3 cm lateral to the transducer will reduce the angle between the needle and the footprint of the transducer (see Figure 6).
- The presence of a motor response to nerve stimulation is useful but not necessary if the nerve, needle, and local anesthetic spread are well visualized.
- Never inject against high resistance because this may signal an intraneural injection (injection pressure must be < 15 psi).
- In the posterior approach to the popliteal nerve block, either an in-plane (lateral or medial) or out-of-plane technique can be used (Figures 9 through 12). While the in-plane lateral approach is commonly used, the advantage of the out-of-plane approach is that the needle path is through the skin and adipose tissue rather than the muscles and thus, less painful.
 or out-of-plane approach are shown - the operator should be able to pick and choose any of these needle orientations, depending on the configuration of tibial and common peroneal branches at the site of injection.")
FIGURE 12. In-plane (lateral or medial) or out-of-plane approach are shown – the operator should be able to pick and choose any of these needle orientations, depending on the configuration of tibial and common peroneal branches at the site of injection.
")
FIGURE 13. Continuous sciatic nerve block in the popliteal fossa using a lateral approach with the patient in the supine position. The needle is positioned within the epineural sheath of the sciatic nerve. After an injection of a small volume of local anesthetic to confirm correct needle position, a catheter is inserted 2–4 cm past the needle tip. Preloading the catheter is useful in facilitating the procedure. (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
CONTINUOUS ULTRASOUND-GUIDED POPLITEAL SCIATIC NERVE BLOCK
The goal of the continuous popliteal sciatic nerve block is to place the catheter within the sciatic nerve sheath in the popliteal fossa (Figure 13). The catheter is inserted 4-5 cm beyond needle tip and its correct placement is documented by observing injection of LA within the sciatic nerve sheath. The catheter is secured either by taping it to the skin or tunneling.
The lateral approach may have some advantage over the prone approach with regard to catheter placement. First, the biceps femoris muscle tends to stabilize the catheter and decrease the chance of dislodgement, compared with the subcutaneous tissue of the popliteal fossa in the prone approach. Second, if the knee is to be flexed and extended, the side of the thigh is less mobile than the back of the knee. Finally, access to the catheter site is more convenient with the lateral approach compared with the prone approach. A common starting infusion regimen is ropivacaine 0.2% at 5 mL/h with a patient-administered bolus of 5 mL every 60 minutes.
Follow the link to Continuous Peripheral Nerve Blocks for additional information.
This text is a sample of content from the Compendium of Regional Anesthesia on the NYSORA LMS.
NYSORA’s Compendium of Regional Anesthesia is simply the most comprehensive, and practical curriculum on Regional Anesthesia from A to Z, featuring NYSORA’s Premium content. As opposed to textbooks and e-books, the Compendium is continuously updated and features NYSORA’s newest videos, animations, and visual content.
The Compendium is one of several gold-standard educational courses on NYSORA’s Learning System (the NYSORA LMS), and registration to NYSORALMS.com is free. The FULL access to the Compendium, however, is based on an annual subscription, as it requires an army of illustrators, video editors, and an educational team to continue making it the BEST tool for education on everything regional anesthesia. While you can think of the compendium as an ebook on steroids, a quick test drive will give you a real-time feel of how incredible the Compendium really is. Your subscription will transform the way you read about regional anesthesia:
- Learn visually: Everything regional, including spinal, epidural, and nerve block procedures and management protocols
- Review step-by-step techniques instructions for over 60 nerve blocks
- Access NYSORA’s fabled illustrations, animations, and videos (such as Reverse Ultrasound Anatomy)
- Access RA info on any device via the desktop platform and mobile app
- Get real-time updates
- Review infographics for exam preparation (e.g. EDRA)
- Use the Community feed with real case discussions, images and videos are posted and discussed by subscribers and world’s top experts alike.
Even if you do not wish to subscribe to the Compendium, do register to the NYSORA LMS, be the first to know what’s new in regional anesthesia, and get involved in case discussions.
Here’s what the activity feed on NYSORA LMS looks like:
We are convinced that once you experience the Compendium on the NYSORA LMS, and you’ll never go back to your old books, and your subscription will support keeping NYSORA.com free for the rest of the world.
Additional Reading
- Sala-Blanch X, López A, Prats-Galino A: Vloka sciatic nerve sheath: a tribute to a visionary. Reg Anesth Pain Med 2015;40:174.
- Prasad NK, Capek S, de Ruiter GC, Amrami KK, Spinner RJ: The subparaneurial compartment: a new concept in the clinico-anatomic classification of peripheral nerve lesions. Clin Anat 2015;28:925–930.
- Tiyaprasertkul W, Bernucci F, González AP, et al: A randomized comparison between single- and triple-injection subparaneural popliteal sciatic nerve block. Reg Anesth Pain Med 2015;40:315–320.
- Choquet O, Noble GB, Abbal B, Morau D, Bringuier S, Capdevila X: Subparaneural versus circumferential extraneural injection at the bifurcation level in ultrasound-guided popliteal sciatic nerve blocks: a prospective, randomized, double-blind study. Reg Anesth Pain Med 2014;39:306–311.
- Sala-Blanch X, Reina MA, Ribalta T, Prats-Galino A: Sciatic nerve structure and nomenclature: epineurium to paraneurium: is this a new paradigm? Reg Anesth Pain Med 2013;38:463–465.
- Karmakar MK, Shariat AN, Pangthipampai P, Chen J: High-definition ultrasound imaging defines the paraneural sheath and the fascial compartments surrounding the sciatic nerve at the popliteal fossa. Reg Anesth Pain Med 2013;38:447–451.
- Lopez AM, Sala-Blanch X, Castillo R, Hadzic A: Ultrasound-guided injection inside the common sheath of the sciatic nerve at division level has a higher success rate than an injection outside the sheath. Rev Esp Anestesiol Reanim 2014;61:304–310.
- Perlas A, Wong P, Abdallah F, Hazrati LN, Tse C, Chan V: Ultrasound-guided
- popliteal nerve block through a common paraneural sheath versus conventional injection: a prospective, randomized, double-blind study. Reg Anesth Pain Med 2013;38:218–225.
- Ip V, Tsui B: Injection through the paraneural sheath rather than circumferential spread facilitates safe, effective sciatic nerve block. Reg Anesth Pain Med 2013;38:373.
- Endersby R, Albrecht E, Perlas A, Chan V: Semantics, misnomer, or uncertainty: where is the epineurium on ultrasound? Reg Anesth Pain Med 2012;37:360–361.
- Tran DQ, Dugani S, Pham K, Al-Shaafi A, Finlayson RJ: A randomized comparison between subepineural and conventional ultrasound-guided popliteal sciatic nerve block. Reg Anesth Pain Med 2011;36:548–552.
- Sala-Blanch X, López AM, Pomés J, Valls-Sole J, García AI, Hadzic A: No clinical or electrophysiologic evidence of nerve injury after intraneural injection during sciatic popliteal nerve block. Anesthesiology 2011;115: 589–595.
- Morau D, Levy F, Bringuier S, et al: Ultrasound-guided evaluation of the local anesthetic spread parameters required for a rapid surgical popliteal sciatic nerve block. Reg Anesth Pain Med 2010;35:559–564.
- Vloka JD, Hadzić A, Lesser JB, et al: A common epineural sheath for the nerves in the popliteal fossa and its possible implications for sciatic nerve block. Anesth Analg 1997;84:387–390.
- Choquet O, Capdevila X: Ultrasound-guided nerve blocks: the real position of the needle should be defined. Anesth Analg 2012;114: 929–930.
- Sinha SK, Abrams JH, Arumugam S, et al: Femoral nerve block with selective tibial nerve block provides effective analgesia without foot drop after total knee arthroplasty: a prospective, randomized, observer-blinded study. Anesth Analg 2012;115:202–206.
- Ting PH, Antonakakis JG, Scalzo DC: Ultrasound-guided common peroneal nerve block at the level of the fibular head. J Clin Anesth 2012;24:145–147.
- Aguirre J, Perinola L, Borgeat A: Ultrasound-guided evaluation of the local anesthetic spread parameters required for a rapid surgical popliteal sciatic nerve block. Reg Anesth Pain Med 2011;36:308–309.
- Aguirre J, Ruland P, Ekatodramis G, Borgeat A: Ultrasound versus neurostimulation for popliteal nerve block: another vain effort to show a nonexisting clinical relevant difference. Anaesth Intensive Care 2009;37: 665–666.
- Aguirre J, Valentin Neudorfer C, Ekatodramis G, Borgeat A: Ultrasound guidance for sciatic nerve block at the popliteal fossa should be compared with the best motor response and the lowest current clinically used in neurostimulation technique. Reg Anesth Pain Med 2009;34:182–183.
- Anderson JG, Bohay DR, Maskill JD, et al: Complications after popliteal nerve block for foot and ankle surgery. Foot Ankle Int 2015;36:1138–1143.
- Barbosa FT, Barbosa TR, da Cunha RM, Rodrigues AK, Ramos FW, de Sousa-Rodrigues CF: Bases anatômicas para o bloqueio anestésico do nervo isquiático no nível do joelho. [Anatomical basis for sciatic nerve block at the knee level.] Braz J Anesthesiol 2015;65:177–179.
- Barrington MJ, Lai SL, Briggs CA, Ivanusic JJ, Gledhill SR: Ultrasound-guided midthigh sciatic nerve block—a clinical and anatomical study. Reg Anesth Pain Med 2008;33:369–376.
- Bendtsen TF, Nielsen TD, Rohde CV, Kibak K, Linde F: Ultrasound guidance improves a continuous popliteal sciatic nerve block when compared with nerve stimulation. Reg Anesth Pain Med 2011;36:181–184.
- Birch MD, Matthews JL, Galitzine SV: Patient and needle positioning during popliteal nerve block. Reg Anesth Pain Med 2013;38:253.
- Børglum J, Johansen K, Christensen MD, et al: Ultrasound-guided single-penetration dual-injection block for leg and foot surgery: a prospective, randomized, double-blind study. Reg Anesth Pain Med 2014;39: 18–25.
- Bruhn J, van Geffen GJ, Gielen MJ, Scheffer GJ: Visualization of the course of the sciatic nerve in adult volunteers by ultrasonography. Acta Anaesthesiol Scand 2008;52:1298–1302.
- Brull R, Macfarlane AJ, Parrington SJ, Koshkin A, Chan VW: Is circumferential injection advantageous for ultrasound-guided popliteal sciatic nerve block? A proof-of-concept study. Reg Anesth Pain Med 2011;36:266–270.
- Buys MJ, Arndt CD, Vagh F, Hoard A, Gerstein N: Ultrasound-guided sciatic nerve block in the popliteal fossa using a lateral approach: onset time comparing separate tibial and common peroneal nerve injections versus injecting proximal to the bifurcation. Anesth Analg 2010;110:635–637.
- Cataldo R, Carassiti M, Costa F, et al: Starting with ultrasonography decreases popliteal nerve block performance time in inexperienced hands: a prospective randomized study. BMC Anesthesiol 2012;12:33.
- Chin KJ, Perlas A, Brull R, Chan VW: Ultrasound guidance is advantageous in popliteal nerve block. Anesth Analg 2008;107:2094–2095.
- Clendenen SR, Robards CB, Greengrass RA: Popliteal catheter placement utilizing ultrasound needle guidance system. Local Reg Anesth 2010;3: 45–48.
- Clendenen SR, York JE, Wang RD, Greengrass RA: Three-dimensional ultrasound-assisted popliteal catheter placement revealing aberrant anatomy: implications for nerve block failure. Acta Anaesthesiol Scand 2008;52: 1429–1431.
- Compere V, Cornet C, Fourdrinier V, et al: Thigh abscess as a complication of continuous popliteal sciatic nerve block. Br J Anaesth 2005;95:255–256.
- Creech C, Meyr AJ: Techniques of popliteal nerve regional anesthesia. J Foot Ankle Surg 2013;52:681–685.
- Danelli G, Fanelli A, Ghisi D, et al: Ultrasound vs nerve stimulation multiple injection technique for posterior popliteal sciatic nerve block. Anaesthesia 2009;64:638–642.
- Dufour E, Quennesson P, Van Robais AL, et al: Combined ultrasound and neurostimulation guidance for popliteal sciatic nerve block: a prospective, randomized comparison with neurostimulation alone. Anesth Analg 2008; 106:1553–1558.
- Eisenberg JA, Calligaro KD, Kolakowski S, et al: Is balloon angioplasty of peri-anastomotic stenoses of failing peripheral arterial bypasses worthwhile? Vasc Endovascular Surg 2009;43:346–351.
- Eurin M, Beloeil H, Zetlaoui PJ: A medial approach for a continuous sciatic nerve block in the popliteal fossa [in French]. Can J Anaesth 2006;53: 1165–1166.
- Gallardo J, Lagos L, Bastias C, Henríquez H, Carcuro G, Paleo M: Continuous popliteal nerve block for postoperative analgesia in total ankle arthroplasty. Foot Ankle Int 2012;33:208–212.
- Gartke K, Portner O, Taljaard M: Neuropathic symptoms following continuous popliteal nerve block after foot and ankle surgery. Foot Ankle Int 2012;33: 267–274.
- Germain G, Lévesque S, Dion N, et al: Brief reports: a comparison of an injection cephalad or caudad to the division of the sciatic nerve for ultrasound-guided popliteal nerve block: a prospective randomized study. Anesth Analg 2012;114:233–235.
- Gray AT, Huczko EL, Schafhalter-Zoppoth I: Lateral popliteal nerve block with ultrasound guidance. Reg Anesth Pain Med 2004;29:507–509.
- Gucev G, Karandikar K, Charlton T: Midcalf continuous peripheral nerve block anesthesia for hallux valgus surgery: case report. Foot Ankle Int 2014;35:175–177.
- Gurkan Y, Sarisoy HT, Caglayan C, Solak M, Toker K: “Figure of four” position improves the visibility of the sciatic nerve in the popliteal fossa. Agri 2009;21:149–154.
- Harvey S, Corey J, Townley K: A modification of the single-penetration, dual-injection technique for combined sciatic and saphenous nerve blocks. Reg Anesth Pain Med 2014;39:561.
- Hegewald K, McCann K, Elizaga A, Hutchinson BL: Popliteal nerve blocks for foot and ankle surgery: success rate and contributing factors. J Foot Ankle Surg 2014;53:176–178.
- Huntoon MA, Huntoon EA, Obray JB, Lamer TJ: Feasibility of ultrasound-guided percutaneous placement of peripheral nerve stimulation electrodes in a cadaver model: part one, lower extremity. Reg Anesth Pain Med 2008; 33:551–557.
- Ilfeld BM, Sandhu NS, Loland VJ, et al: Common peroneal nerve compression by a popliteal venous aneurysm. Am J Phys Med Rehabil 2009;88:947–950.
- Jeong JS, Shim JC, Jeong MA, Lee BC, Sung IH: Minimum effective anaesthetic volume of 0.5% ropivacaine for ultrasound-guided popliteal sciatic nerve block in patients undergoing foot and ankle surgery: determination of ED50 and ED95. Anaesth Intensive Care 2015;43:92–97.
- Karmakar M, Li X, Li J, Sala-Blanch X, Hadzic A, Gin T: Three-dimensional/four-dimensional volumetric ultrasound imaging of the sciatic nerve. Reg Anesth Pain Med 2012;37:60–66.
- Khabiri B, Arbona F, Norton J: “Gapped supine” position for ultrasound-guided lateral popliteal fossa nerve block of the sciatic nerve. Anesth Analg 2007;105:1519.
- Khabiri B, Hamilton C, Norton J, Arbona F: Ultrasound-guided supine posterior approach for popliteal sciatic nerve block. J Clin Anesth 2012;24:680.
- Koscielniak-Nielsen ZJ, Rasmussen H, Hesselbjerg L: Long-axis ultrasound imaging of the nerves and advancement of perineural catheters under direct vision: a preliminary report of four cases. Reg Anesth Pain Med 2008;33:477–482.
- Maalouf D, Liu SS, Movahedi R, et al: Nerve stimulator versus ultrasound guidance for placement of popliteal catheters for foot and ankle surgery. J Clin Anesth 2012;24:44–50.
- Mariano ER, Cheng GS, Choy LP, et al: Electrical stimulation versus ultrasound guidance for popliteal-sciatic perineural catheter insertion: a randomized controlled trial. Reg Anesth Pain Med 2009;34:480–485.
- Mariano ER, Loland VJ, Sandhu NS, et al: Comparative efficacy of ultrasound-guided and stimulating popliteal-sciatic perineural catheters for postoperative analgesia. Can J Anaesth 2010;10:919–926.
- Minville V, Zetlaoui PJ, Fessenmeyer C, Benhamou D: Ultrasound guidance for difficult lateral popliteal catheter insertion in a patient with peripheral vascular disease. Reg Anesth Pain Med 2004;29:368–370.
- Missair A, Weisman RS, Suarez MR, Yang R, Gebhard RE: A 3-dimensional ultrasound study of local anesthetic spread during lateral popliteal nerve block: what is the ideal endpoint for needle tip position? Reg Anesth Pain Med 2012;37:627–632.
- Morau D, Levy F, Bringuier S, et al: Ultrasound-guided evaluation of the local anesthetic spread parameters required for a rapid surgical popliteal sciatic nerve block. Reg Anesth Pain Med 2010;35:559–564.
- Orebaugh SL, Bigeleisen PE, Kentor ML: Impact of a regional anesthesia rotation on ultrasonographic identification of anatomic structures by anesthesiology residents. Acta Anaesthesiol Scand 2009;53:364–368.
- Orebaugh SL, Williams BA, Vallejo M, Kentor ML: Adverse outcomes associated with stimulator-based peripheral nerve blocks with versus without ultrasound visualization. Reg Anesth Pain Med 2009;34: 251–255.
- Perkins JM: Standard varicose vein surgery. Phlebology 2009;24(Suppl 1):34–41.
- Perlas A, Brull R, Chan VW, McCartney CJ, Nuica A, Abbas S: Ultrasound guidance improves the success of sciatic nerve block at the popliteal fossa. Reg Anesth Pain Med 2008;33:259–265.
- Perlas A, Chan VW, Brull R: Several “correct” approaches to nerve stimulatorguided popliteal fossa nerve block. Reg Anesth Pain Med 2009;34:624–625.
- Prakash, Bhardwaj AK, Devi MN, Sridevi NS, Rao PK, Singh G: Sciatic nerve division: a cadaver study in the Indian population and review of the literature. Singapore Med J 2010;51:721–723.
- Prasad A, Perlas A, Ramlogan R, Brull R, Chan V: Ultrasound-guided popliteal nerve block distal to sciatic nerve bifurcation shortens onset time: a prospective randomized double-blind study. Re Anesth Pain Med 2010;35: 267–271.
- Reinoso-Barbero F, Saavedra B, Segura-Grau E, Llamas A: Anatomical comparison of sciatic nerves between adults and newborns: clinical implications for ultrasound-guided nerve block. J Anat 2014;224:108–112.
- Robards C, Hadžić A, Somasundaram L, et al: Intraneural injection with low-current stimulation during popliteal sciatic nerve block. Anesth Analg 2009;109:673–677.
- Robards CB, Porter SB, Logvinov I, Clendenen SR: Success of ultrasound-guided popliteal sciatic nerve catheters is not influenced by nerve stimulation. Middle East J Anaesthesiol 2013;22:179–183.
- Sala-Blanch X, de Riva N, Carrera A, López AM, Prats A, Hadzic A: Ultrasound-guided popliteal sciatic nerve block with a single injection at the sciatic division results in faster nerve block onset than the classical nerve stimulator technique. Anesth Analg 2012;114:1121–1127.
- Sala Blanch X, Lopez AM, Carazo J, et al: Intraneural injection during nerve stimulator-guided sciatic nerve block at the popliteal fossa. Br J Anaesth 2009;102:855–861.
- Schwartz AK, Lee DK: Ultrasound-guided (needle-in-plane) perineurial catheter insertion: the effect of catheter-insertion distance on postoperative analgesia. Reg Anesth Pain Med 2011;36:261–265.
- Sinha A, Chan VW: Ultrasound imaging for popliteal sciatic nerve block. Reg Anesth Pain Med 2004;29:130–134.
- Sit M, Higgs JB: Non-popliteal synovial rupture. J Clin Rheumatol 2009;15:185–189.
- Sites BD, Gallagher J, Sparks M: Ultrasound-guided popliteal nerve block demonstrates an atypical motor response to nerve stimulation in 2 patients with diabetes mellitus. Reg Anesth Pain Med 2003;28:479–482.
- Sites BD, Gallagher JD, Tomek I, Cheung Y, Beach ML: The use of magnetic resonance imaging to evaluate the accuracy of a handheld ultrasound machine in localizing the sciatic nerve in the popliteal fossa. Reg Anesth Pain Med 2004;29:413–416.
- Techasuk W, Bernucci F, Cupido T, et al: Minimum effective volume of combined lidocaine-bupivacaine for analgesic subparaneural popliteal sciatic nerve block. Reg Anesth Pain Med 2014;39:108–111.
- Tiyaprasertkul W, Bernucci F, González AP, et al: A randomized comparison between single- and triple-injection subparaneural popliteal sciatic nerve block. Reg Anesth Pain Med 2015;40:315–320.
- Tran DQ, González AP, Bernucci F, Pham K, Finlayson RJ: A randomized comparison between bifurcation and pre-bifurcation subparaneural popliteal sciatic nerve blocks. Anesth Analg 2013;116:1170–1175.
- Tsui BC, Finucane BT: The importance of ultrasound landmarks: a “traceback” approach using the popliteal blood vessels for identification of the sciatic nerve. Reg Anesth Pain Med 2006;31:481–482.
- Tuveri M, Borsezio V, Argiolas R, Medas F, Tuveri A: Ultrasonographic venous anatomy at the popliteal fossa in relation to tibial nerve course in normal and varicose limbs. Chir Ital 2009;61:171–177.
- van Geffen GJ, van den Broek E, Braak GJ, Giele JL, Gielen MJ, Scheffer GJ: A prospective randomized controlled trial of ultrasound-guided versus nerve stimulation-guided distal sciatic nerve block at the popliteal fossa. Anaesth Intensive Care 2009;37:32–37.
- Verelst P, van Zundert A: Ultrasound-guided popliteal nerve block shortens onset time compared to pre-bifurcation sciatic nerve block. Reg Anesth Pain Med 2010;35:565–566.
Continue reading Ultrasound-Guided Sciatic Nerve Block