Thomas F. Bendtsen, Ana M. Lopez, and Thomas B. Clark
FACTS
• Indications: saphenous vein stripping or harvesting; supplementation for medial foot/ankle surgery in combination with a sciatic nerve block, and analgesia for knee surgery in combination with multimodal analgesia.
• Transducer position: transverse on the anteromedial thigh at the junction between the middle and distal third of the thigh or below the knee at the level of the tibial tuberosity, depending on the approach chosen (proximal or distal) (Figure 1)
• Goal: local anesthetic spread lateral to the femoral artery and deep to the sartorius muscle or more distal, below the knee, adjacent to the saphenous vein.
• Local anesthetic: 5–10 mL
FIGURE 1. Transducer position and needle insertion to nerve block the saphenous nerve (A) at the level of the lower third of the thigh and (B) below the knee.
GENERAL CONSIDERATIONS
The saphenous nerve is a terminal sensory branch of the femoral nerve. It supplies innervation to the medial aspect of the leg down to the ankle and foot. It also sends infrapatellar branches to the knee joint. A saphenous nerve block is useful as a supplement to sciatic nerve block for foot and ankle procedures that involve the medial aspect of the malleolus and the foot. The nerve block has also been reported as a supplement to multimodal analgesia protocols in patients having knee arthroplasty. Typically, a more proximal (mid-thigh) approach and a larger volume of local anesthetic is used for this “adductor canal nerve block”. Several approaches have been described to nerve block the saphenous nerve along its route from the inguinal area to the medial malleolus (Figure 2). The use of ultrasound (US) guidance has improved the success rates of the saphenous nerve blocks compared with field nerve blocks below the knee and blind trans-sartorial approaches.
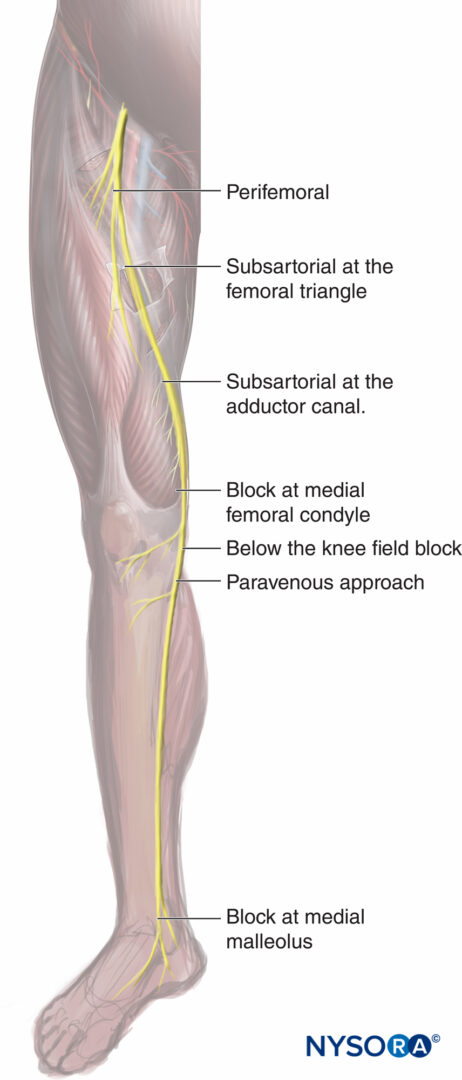
FIGURE 2. Various approaches to the saphenous nerve block: the perifemoral typically targets the nerve to the vastus medialis muscle with nerve stimulation; the subsartorial at the femoral riangle; subsartorial at the adductor canal; at the medial femoral condyle, between the tendons of the sartorius and the gracilis muscle; once the femoral vessels have crossed the adductor hiatus to become the popliteal vessels; the paravenous approach using the saphenous vein as a landmark at the level of the tibial tuberosity; and at the level of the medial malleolus.
ULTRASOUND ANATOMY
The sartorius muscle descends in a lateral to the medial direction across the anterior thigh and forms a “roof ” over the adductor canal in the lower half of the thigh. The muscle appears as a trapezoid shape beneath the subcutaneous layer of adipose tissue.
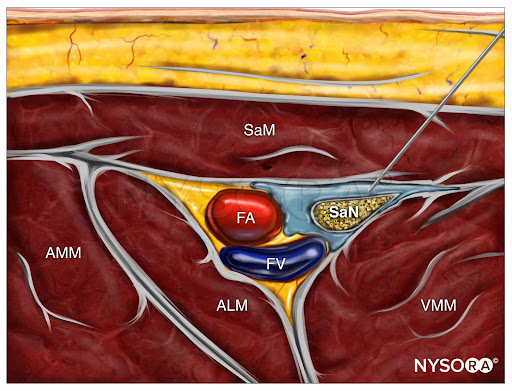
The sides of the triangular canal are formed by the vastus medialis laterally and the adductor longus or magnus medially (depending on how proximal or distal the scan is). The saphenous nerve is typically imaged by ultrasound as a small, round, hyperechoic structure anterior to the artery. The femoral vein accompanies the artery and saphenous nerve, which all can be identified at a depth of 2–3 cm (Figure 3).
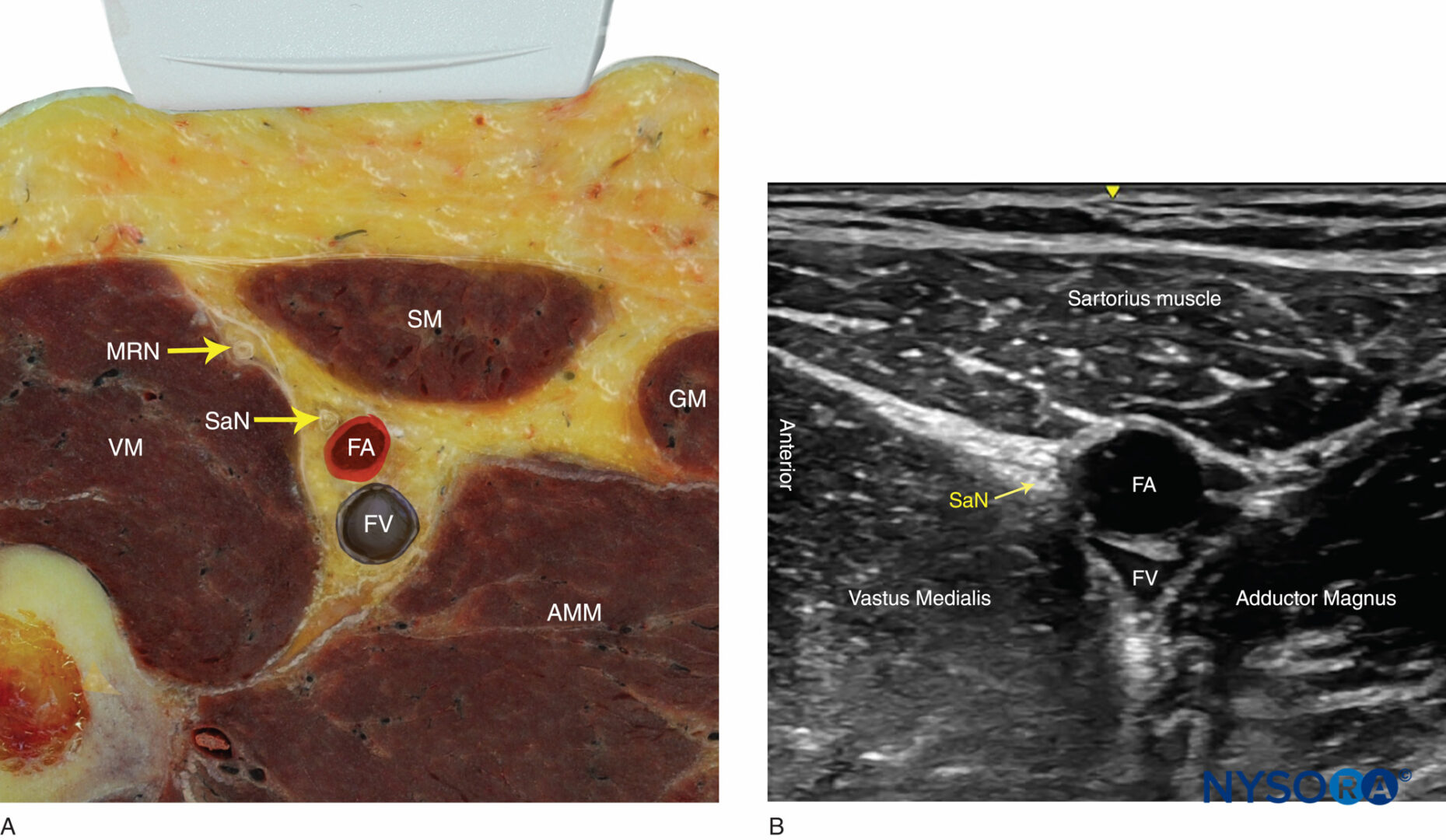
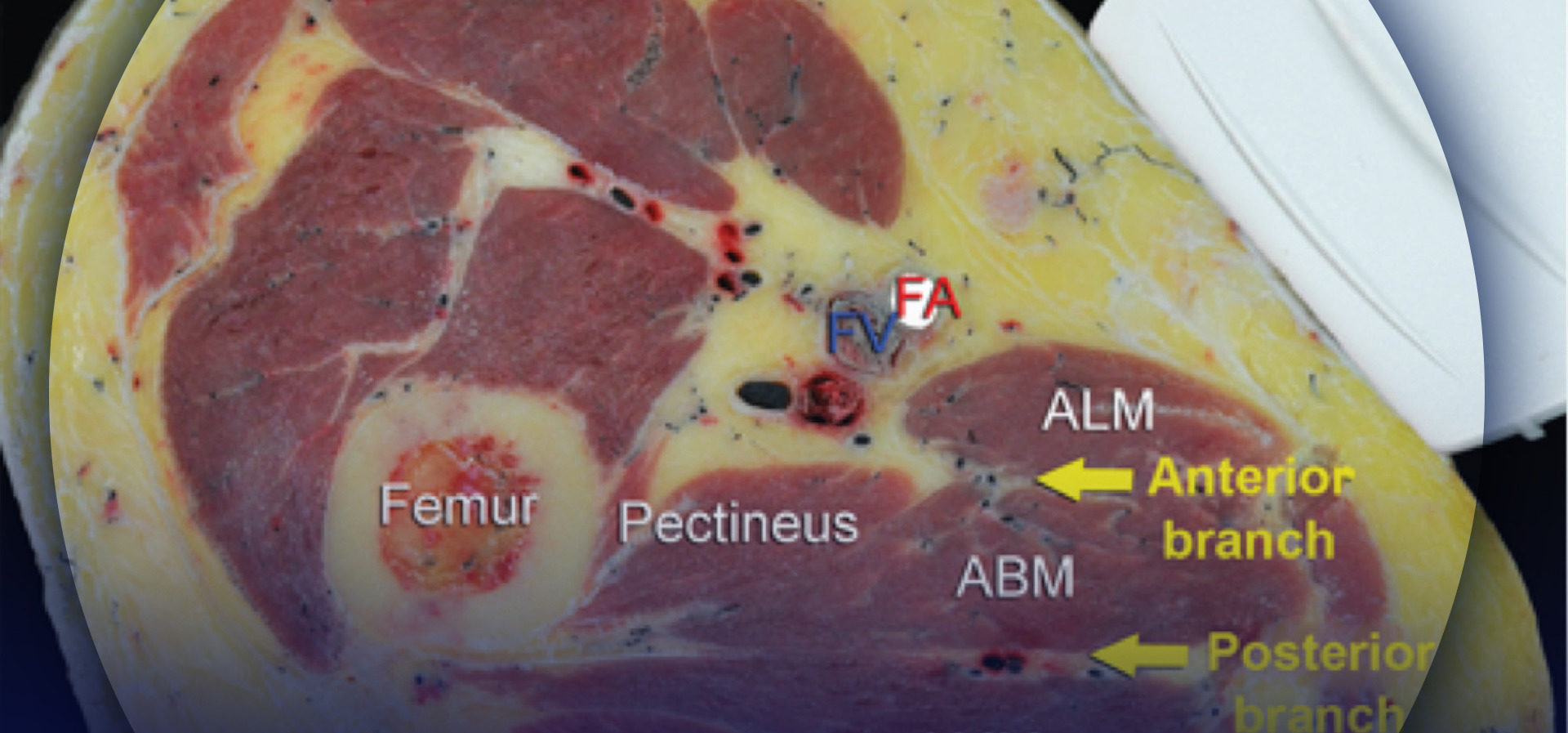
FIGURE 3. (A) Cross-sectional anatomy of the saphenous nerve at the level of the thigh. The saphenous nerve (SaN) is positioned between the sartorius muscle (SM) and the vastus medialis muscle (VM), anterolateral to the femoral artery (FA) and vein (FV). AMM, adductor magnus muscles; GM, gracilis muscle; MRN, medial retinacular nerve. (B) US anatomy of the subsartorial space at the midthigh.
When attempting to identify the saphenous nerve on US image, the following anatomical considerations should be kept in mind:
- Above the knee: The saphenous nerve pierces the fascia lata between the tendons of the sartorius and gracilis muscles before becoming a subcutaneous nerve.
- The saphenous nerve lies in close proximity to several vessels along its trajectory: the femoral artery above the knee, the descending genicular artery and its saphenous branch at the knee, and the great saphenous vein in the lower leg and ankle.
- Below the knee, the saphenous nerve passes along the tibial side of the leg, adjacent to the great saphenous vein subcutaneously (Figure 4).
- At the ankle, branches of the saphenous nerve are located medially, next to the subcutaneously positioned saphenous vein.
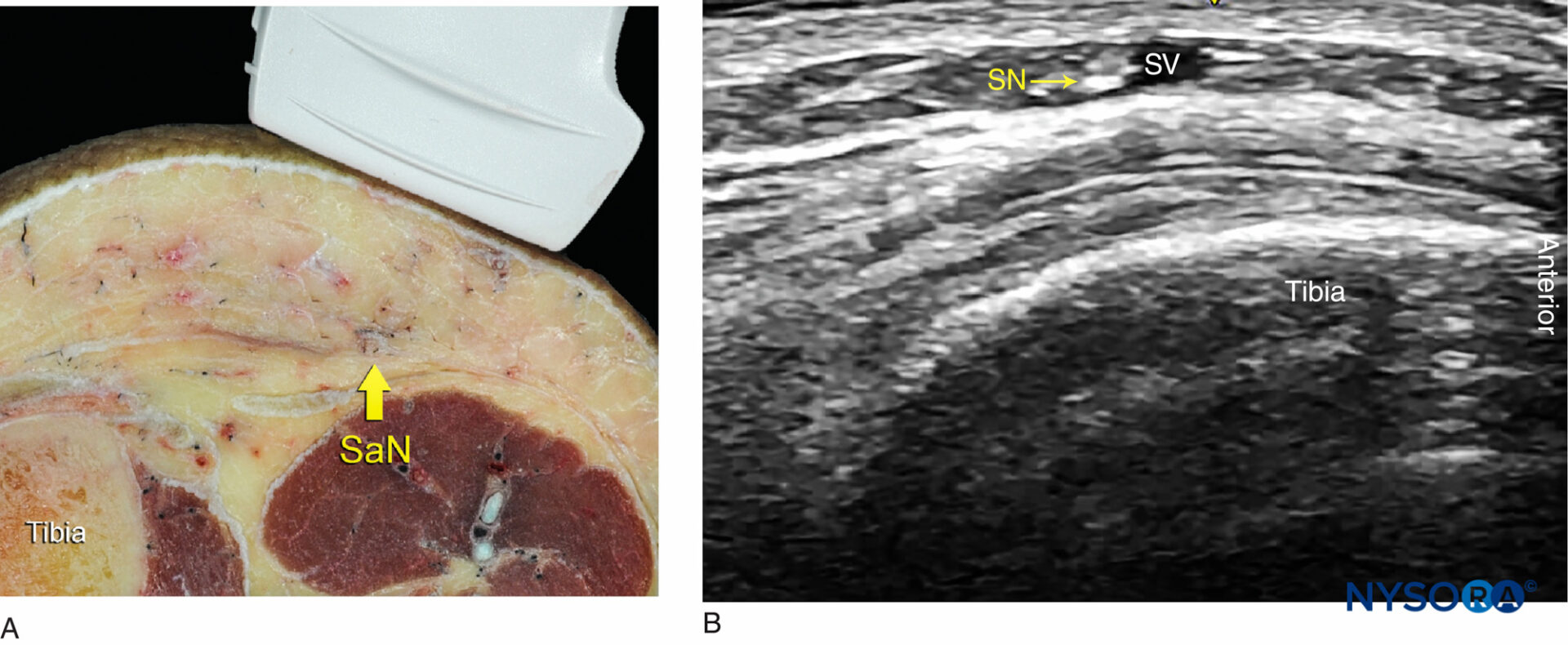
FIGURE 4. (A) Cross-sectional anatomy of the saphenous nerve (SaN) at the level of the tibial tuberosity. (B) US image of the SaN below the knee. The SaN is seen within the immediate vicinity of the great saphenous vein (SV). The transducer should be applied lightly to avoid compression of the SV because the vein serves as an important landmark for the technique.
From the Compendium of Regional Anesthesia: Cognitive priming for an adductor canal block.
DISTRIBUTION OF ANESTHESIA
The saphenous nerve block results in anesthesia of the skin on the medial leg and foot (Figure 5). For a more comprehensive review of the femoral and saphenous nerve distributions, see Functional Regional Anesthesia Anatomy. Of note, although the saphenous nerve block is a sensory nerve block, an injection of a large volume of local anesthetic into the subsartorial space can result in a partial motor nerve block of the vastus medialis due to the nerve block of the femoral nerve branch to this muscle, often contained in the canal. For this reason, caution must be taken when advising patients regarding the safety of unsupported ambulation after undergoing a proximal saphenous nerve block.
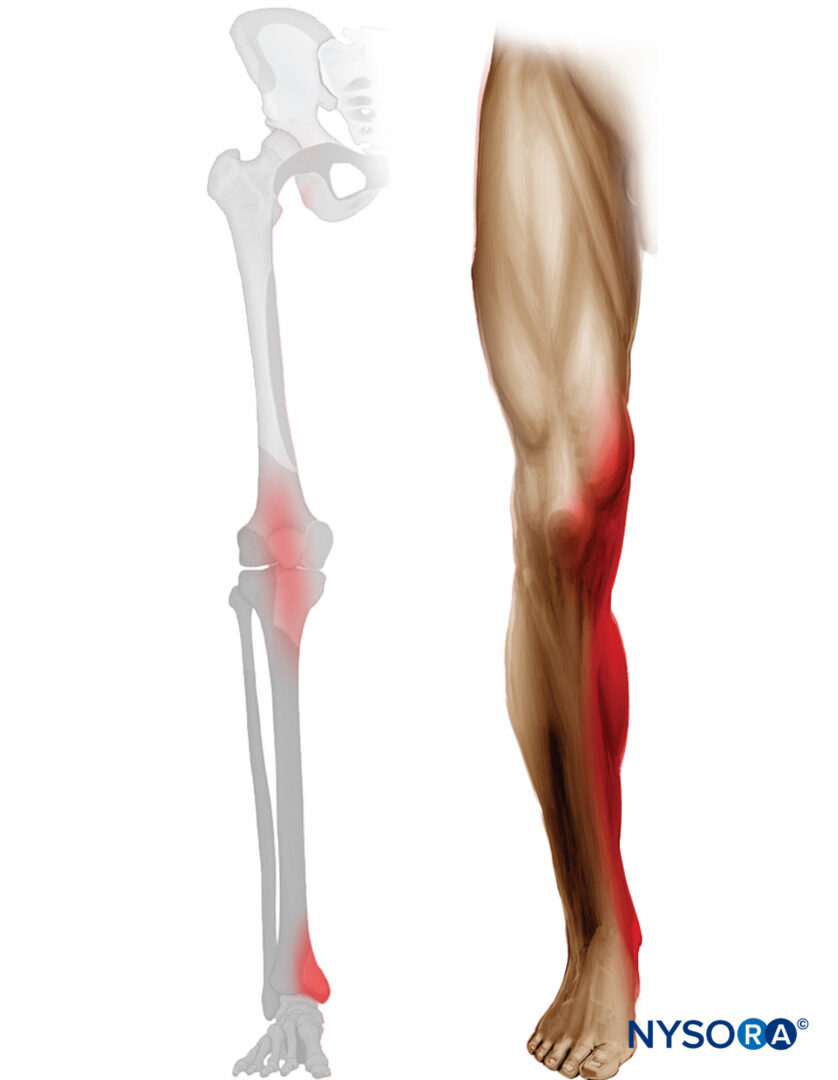
FIGURE 5. Expected distribution of analgesia after saphenous nerve block at the level of midthigh.
EQUIPMENT
- Ultrasound machine with a linear transducer (8–14 MHz), sterile sleeve, and gel
- Standard nerve block tray
- One 10-mL syringe containing local anesthetic
- An 80 mm 22-25 gauge needle
- Peripheral nerve stimulator to elicit paresthesia
- Sterile gloves
Learn more about Equipment for Peripheral Nerve Blocks here.
LANDMARKS AND PATIENT POSITIONING FOR THE PROXIMAL APPROACH
The patient is placed in any position that allows for comfortable placement of the US transducer and needle advancement. This nerve block typically is performed with the patient in the supine position, with the thigh abducted and externally rotated to allow access to the medial thigh (see Figure 1a).
GOAL
The goal is to place the needle tip just anterior to the femoral artery, deep to the sartorius muscle, and to deposit 5–10 mL (or up to 20 mL for the adductor canal nerve block) of local anesthetic until its spread around the artery is confirmed with US visualization. Nerve Block of the nerve at other, more distal and superficial locations consists of a simple subcutaneous infiltration of the tissues within the immediate vicinity of the nerve under US guidance.
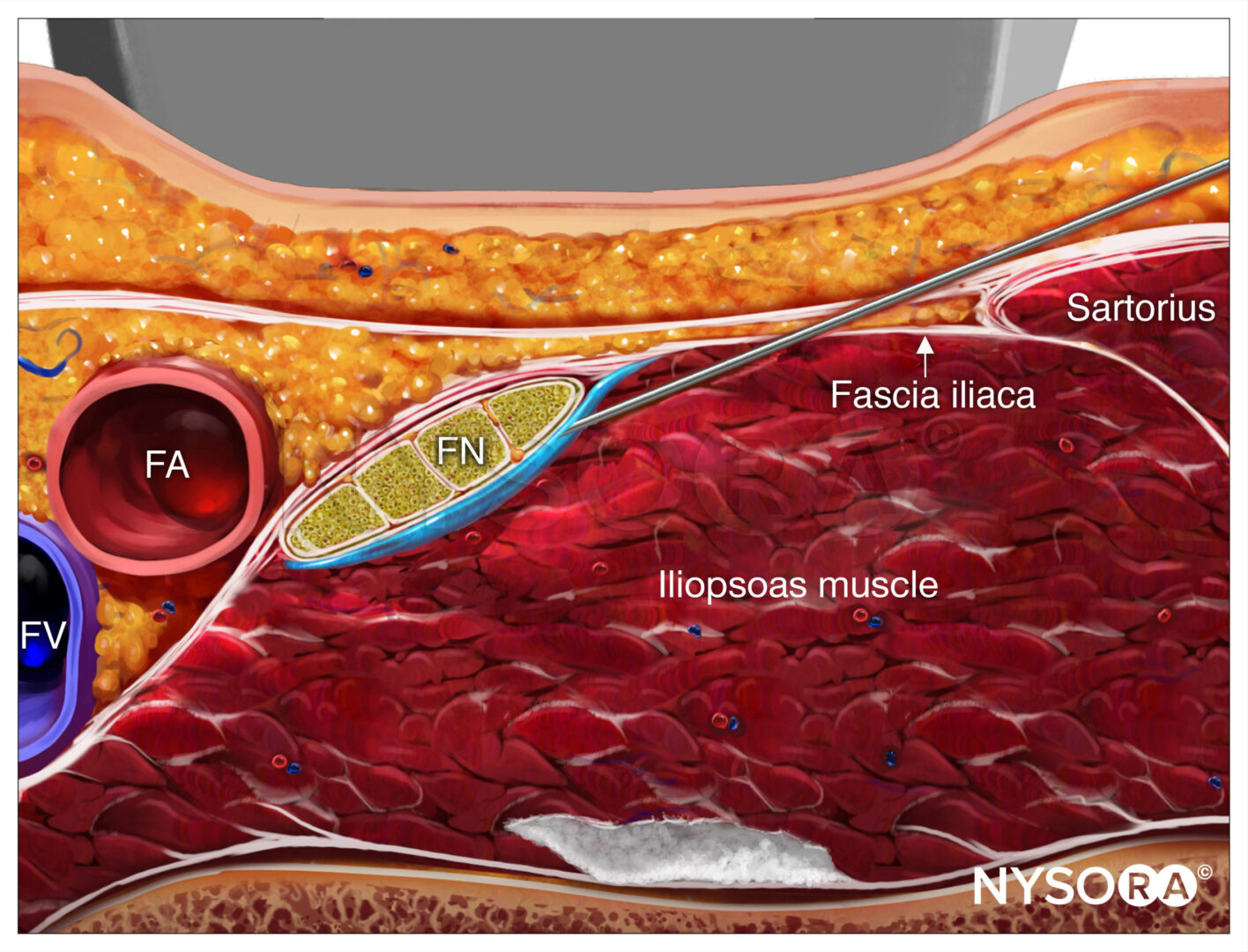
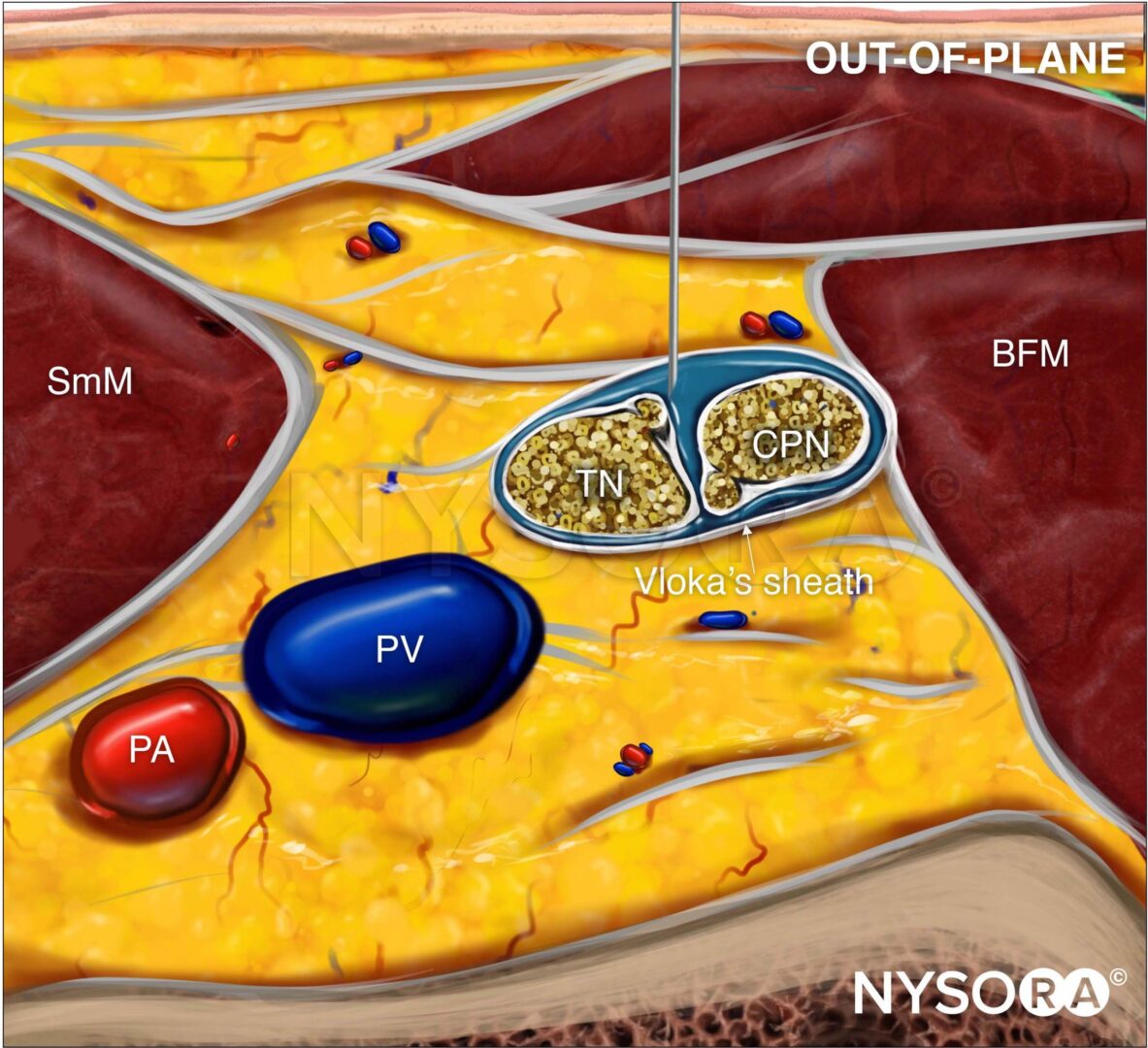
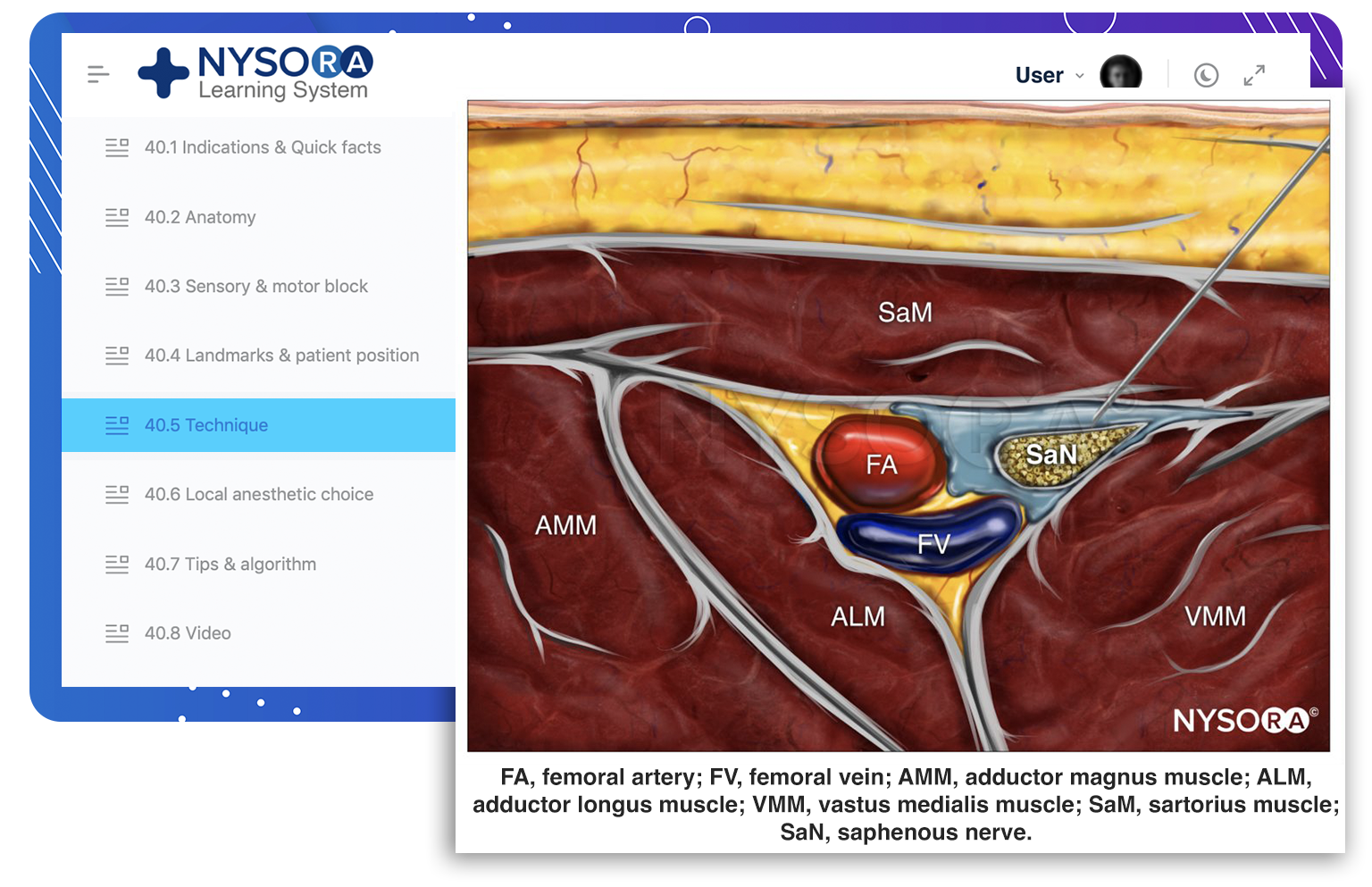
From the Compendium of Regional Anesthesia: Reverse Ultrasound Anatomy for an adductor canal block with needle insertion in-plane and local anesthetic spread (blue). FA, femoral artery; FV, femoral vein; AMM, adductor magnus muscle; ALM, adductor longus muscle; VMM, vastus medialis muscle; SaM, sartorius muscle; SaN, saphenous nerve.
TECHNIQUE
The skin is disinfected and the transducer is placed anteromedially, approximately at the junction between the middle and distal third of the thigh or somewhat lower. If the artery is not immediately obvious, several maneuvers can be used to identify it, including color Doppler scanning to trace the femoral artery caudally from the inguinal crease. Once the femoral artery has been identified, the probe is moved distally to trace the artery until it passes through the adductor hiatus to become the popliteal artery.
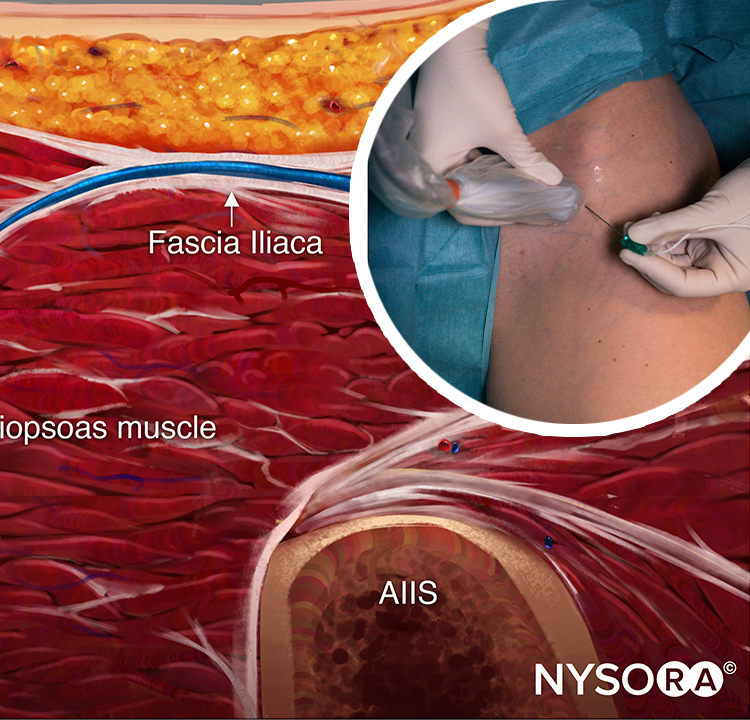
The saphenous nerve block should be performed at the most distal level where the artery still lies immediately deep to the sartorius muscle, thus minimizing the amount of motor nerve block of the vastus medialis; an adductor canal nerve block is typically performed more proximally, around the mid-thigh level. The needle is inserted in-plane in a lateral-to-medial orientation and advanced toward the femoral artery (Figure 1a and 6). If nerve stimulation is used (1 mA, 1 msec), the passage of the needle through the sartorius and/or adductor muscles and into the adductor canal is usually associated with paresthesia in the saphenous nerve distribution. Once the needle tip is visualized anterior to the artery and after careful aspiration, 1–2 mL of local anesthetic is injected to confirm the proper injection site (Figure 6). When injection of local anesthetic does not appear to result in its spread around the femoral artery, additional needle repositions and injections may be necessary.
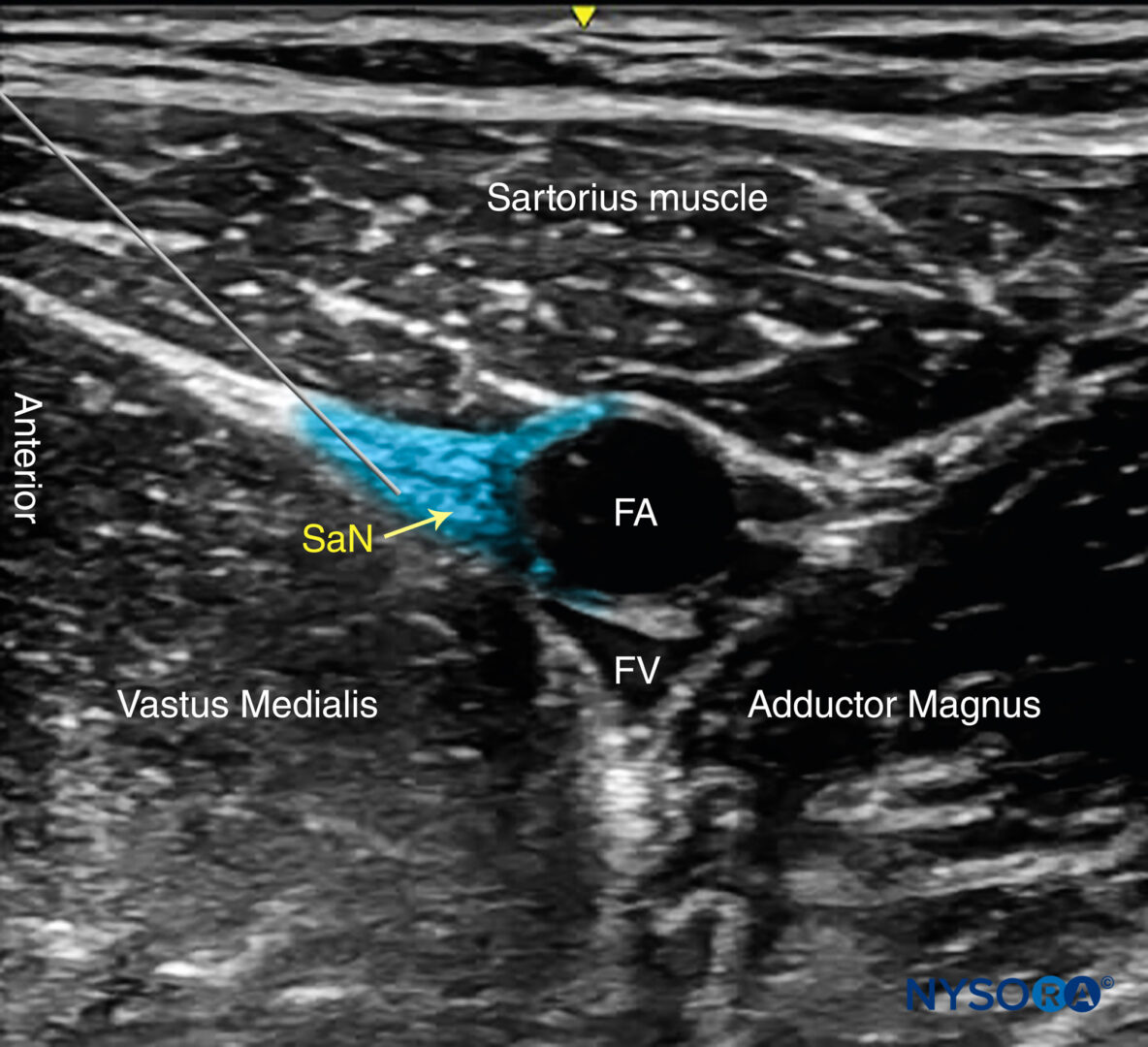
FIGURE 6. Simulated needle path, needle tip position and local anesthetic initial distribution (blue-shaded area) to anesthetize the Saphenous nerve (SaN) at the level of the thigh. FA, femoral artery: FV, femoral vein.
Color Doppler can be used to locate the peri-saphenous branch of the descending geniculate artery in order to avoid puncturing it. Because the saphenous nerve is a purely sensory nerve, high concentrations of local anesthetic are not required and in fact may delay patient ambulation should local anesthetic spread to one of the motor branches of the femoral nerve innervating the quadriceps muscle.
TIPS
- An out-of-plane technique can also be used through the belly of the sartorius muscle. Because the needle tip may not be seen throughout the procedure, small boluses of local anesthetic are administered (0.5–1 mL) as the needle is advanced toward the adductor canal to confirm the location of the needle tip.
- Visualization of the nerve is not necessary for this nerve block, as the saphenous nerve is not always well imaged. Administration of 5–10 mL of local anesthetic next to the artery in the plane between the sartorius and vastus medialis muscles should suffice without confirming nerve position.
- Practitioners should be aware of the potential for partial quadriceps weakness following a more proximal approach along the subsartorial space and/or injection of a large volume (20-30 mL) of local anesthetic. Patient education and assistance with ambulation should be encouraged. For that reason, it is recommended to perform this nerve block as distally as practically possible.
Additional reading Ultrasound-Guided Femoral Nerve Block.
This text is a sample of content from the Compendium of Regional Anesthesia on the NYSORA LMS.
NYSORA’s Compendium of Regional Anesthesia is simply the most comprehensive, and practical curriculum on Regional Anesthesia from A to Z, featuring NYSORA’s Premium content. As opposed to textbooks and e-books, the Compendium is continuously updated and features NYSORA’s newest videos, animations, and visual content.
The Compendium is one of several gold-standard educational courses on NYSORA’s Learning System (the NYSORA LMS), and registration to NYSORALMS.com is free. The FULL access to the Compendium, however, is based on an annual subscription, as it requires an army of illustrators, video editors, and an educational team to continue making it the BEST tool for education on everything regional anesthesia. While you can think of the compendium as an ebook on steroids, a quick test drive will give you a real-time feel of how incredible the Compendium really is. Your subscription will transform the way you read about regional anesthesia:
- Learn visually: Everything regional, including spinal, epidural, and nerve block procedures and management protocols
- Review step-by-step techniques instructions for over 60 nerve blocks
- Access NYSORA’s fabled illustrations, animations, and videos (such as Reverse Ultrasound Anatomy)
- Access RA info on any device via the desktop platform and mobile app
- Get real-time updates
- Review infographics for exam preparation (e.g. EDRA)
- Use the Community feed with real case discussions, images and videos are posted and discussed by subscribers and world’s top experts alike.
Even if you do not wish to subscribe to the Compendium, do register to the NYSORA LMS, be the first to know what’s new in regional anesthesia, and get involved in case discussions.
Here’s what the activity feed on NYSORA LMS looks like:
We are convinced that once you experience the Compendium on the NYSORA LMS, and you’ll never go back to your old books, and your subscription will support keeping NYSORA.com free for the rest of the world.
REFERENCES
- Sahin L, Sahin M, Isikay N: A different approach to an ultrasound-guided saphenous nerve block. Acta Anaesthesiol Scand 2011;55:1030–1031.
- Bendtsen TF, Moriggl B, Chan V, Børglum J. Basic Topography of the Saphenous Nerve in the Femoral Triangle and the Adductor Canal. Reg Anesth Pain Med. 2015;40(4):391–2.
- Davis JJ, Bond TS, Swenson JD: Adductor canal nerve block: more than just the saphenous nerve? Reg Anesth Pain Med 2009;34:618–619.
- Goffin P, Lecoq JP, Ninane V, Brichant JF, Sala-Blanch X, Gautier PE et al. Interfascial Spread of Injectate After Adductor Canal Injection in Fresh Human Cadavers. Anesth Analg. 2016 Aug;123(2):501–3.
- Gray AT, Collins AB: Ultrasound-guided saphenous nerve block. Reg Anesth Pain Med 2003;28:148.
- Head SJ, Leung RC, Hackman GP, Seib R, Rondi K, Schwarz SK: Ultrasound-guided saphenous nerve block–within versus distal to the adductor canal: a proof-of-principle randomized trial. Can J Anaesth 2015;62:37–44.
- Horn JL, Pitsch T, Salinas F, Benninger B: Anatomic basis to the ultrasound-guided approach for saphenous nerve block. Reg Anesth Pain Med 2009;34:486–489.
- Kapoor R, Adhikary SD, Siefring C, McQuillan PM: The saphenous nerve and its relationship to the nerve to the vastus medialis in and around the adductor canal: an anatomical study. Acta Anaesthesiol Scand 2012;56: 365–367.
- Kirkpatrick JD, Sites BD, Antonakakis JG: Preliminary experience with a new approach to performing an ultrasound-guided saphenous nerve block in the mid- to proximal femur. Reg Anesth Pain Med 2010;35:222–223.
- Krombach J, Gray AT: Sonography for saphenous nerve block near the adductor canal. Reg Anesth Pain Med 2007;32:369–370.
- Lundblad M, Kapral S, Marhofer P, et al: Ultrasound-guided infrapatellar nerve block in human volunteers: description of a novel technique. Br J Anaesth 2006;97:710–714.
- Manickam B, Perlas A, Duggan E, Brull R, Chan VW, Ramlogan R: Feasibility and efficacy of ultrasound-guided nerve block of the saphenous nerve in the adductor canal. Reg Anesth Pain Med 2009;34:578–580.
- Marsland D, Dray A, Little NJ, Solan MC: The saphenous nerve in foot and ankle surgery: its variable anatomy and relevance. Foot Ankle Surg 2013;19:76–79.
- Miller BR: Ultrasound-guided proximal tibial paravenous saphenous nerve block in pediatric patients. Paediatr Anaesth 2010;20:1059–1060.
- Pannell WC, Wisco JJ: A novel saphenous nerve plexus with important clinical correlations. Clin Anat 2011;24:994–996.
- Sahin L, Sahin M, Isikay N: A different approach to an ultrasound-guided saphenous nerve block. Acta Anaesthesiol Scand 2011;55:1030–1031.
- Saranteas T, Anagnostis G, Paraskeuopoulos T, et al: Anatomy and clinical implications of the ultrasound-guided subsartorial saphenous nerve block. Reg Anesth Pain Med 2011;36:399–402.
- Tsai PB, Karnwal A, Kakazu C, Tokhner V, Julka IS: Efficacy of an ultrasound-guided subsartorial approach to saphenous nerve block: a case series. Can J Anaesth 2010;57:683–688.
- Tsui BC, Ozelsel T: Ultrasound-guided transsartorial perifemoral artery approach for saphenous nerve block. Reg Anesth Pain Med 2009;34: 177–178.