Paul Hobeika, Tessy Castermans, Joris Duerinckx, and Sam van Boxstael
INTRODUCTION
The wrist block involves anesthesia of the median, ulnar, and radial nerves, including the dorsal sensory branch of the ulnar nerve. The wrist block is simple to perform, essentially devoid of systemic complications, and highly effective for a variety of procedures on the hand and fingers. Wrist blocks can be used in the office or operating room setting. As such, skill in performing a wrist block should be in the armamentarium of every practitioner. A study comparing intra-articular and portal infiltration versus wrist block for analgesia after arthroscopy of the wrist has shown that wrist block provides better and more reliable analgesia in patients undergoing arthroscopy of the wrist without exposing patients to the risk of chondrotoxicity.
INDICATIONS & CONTRAINDICATIONS
A wrist block is most commonly used for hand and finger surgery. The most common hand surgery in the United States is carpal tunnel release. Sir James Paget described carpal tunnel syndrome in 1853. Although Sir James Learmonth reported release of the carpal tunnel at the wrist in 1933, it was not until the 1950s that the surgery became popular through the efforts of George Phalen. Because of the ease of performing a wrist block, wrist blocks are used in a variety of settings including the emergency room, outpatient surgery centers, and office-based anesthesia practices. Hand surgeons rely on the wrist block to perform minor procedures in their offices. A wrist block can be used in a patient with a full stomach requiring emergency surgery, thereby obviating the need for general anesthesia and reducing the risk of aspiration. Although there are only a few contraindications to wrist blocks, local infection at the site of needle insertion and allergy to local anesthetic are the most cited. Patients are usually able to tolerate a tourniquet on the arm without anesthesia for 20 minutes; a wrist tourniquet can be tolerated for about 120 minutes.
FUNCTIONAL ANATOMY OF WRIST BLOCK
Innervation of the hand is shared by the ulnar, median, and radial nerves (Figure 1). The ulnar nerve innervates more intrinsic muscles than the median nerve, and supplies digital branches to the skin of the medial one and a half digits (Figure 2). A corresponding area of the palm is innervated by palmar branches that arise from the ulnar nerve in the forearm. The deep branch of the ulnar nerve accompanies the deep palmar arch and supplies innervation to the three hypothenar muscles, the medial two lumbrical muscles, all the interossei, and the adductor pollicis. The ulnar nerve also innervates the palmaris brevis muscle. The median nerve traverses the carpal tunnel and terminates as digital and recurrent branches. The digital branches innervate the skin of the lateral three and a half digits and, usually, the lateral two lumbrical muscles.
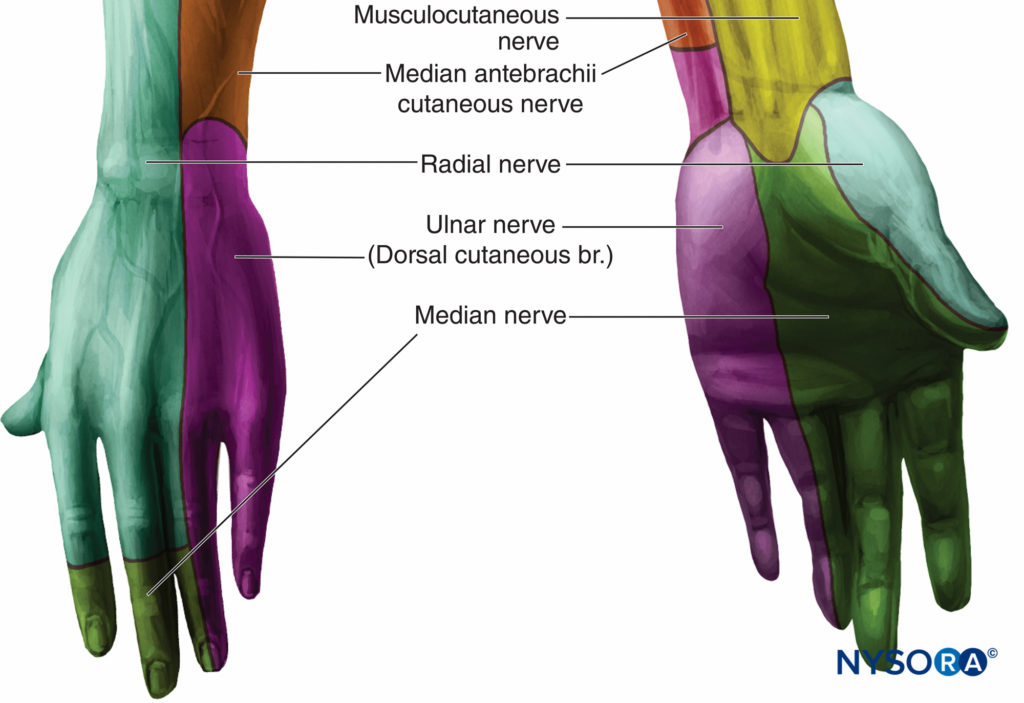
FIGURE 1. Innervation of the hand.
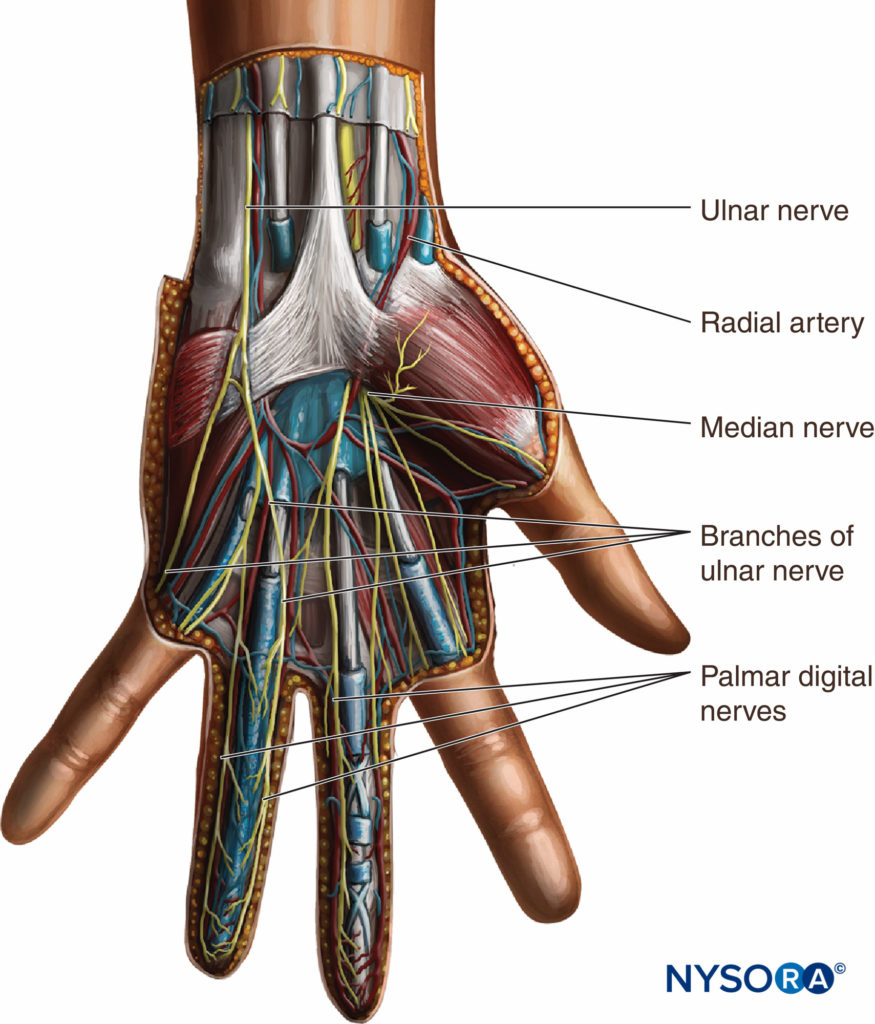
FIGURE 2. Innervation of the hand: The course of the terminal nerves.
A corresponding area of the palm is innervated by palmar branches that arise from the median nerve in the forearm. The recurrent branch of the median nerve supplies the three thenar muscles. In the palm, the digital branches of the ulnar and median nerves lie deep in the superficial palmar arch, but in the fingers, they lie anterior to the digital arteries that arise from the superficial arch. Although the innervation of the ring and middle fingers may vary, the skin on the anterior surface of the thumb is always supplied by the median nerve and that of the little finger by the ulnar nerve. The palmar digital branches of the median and ulnar nerves also innervate the nail beds of their respective digits. The radial nerve passes along the front of the radial side of the forearm. It arises first from the lateral side of the radial artery and beneath the supinator muscle. About 3 in. above the wrist, it leaves the artery, pierces the deep fascia, and divides into two branches (Figure 3). The superficial branch, the smaller of the two branches, supplies the skin of the radial side and base of the thumb and joins the anterior branch of the musculocutaneous nerve. The deep branch of the radial nerve communicates with the posterior branch of the musculocutaneous nerve. On the dorsum of the hand, the deep branch of the radial nerve forms an arch with the dorsal cutaneous branch of the ulnar nerve.
Learn more about Functional Regional Anesthesia Anatomy here.
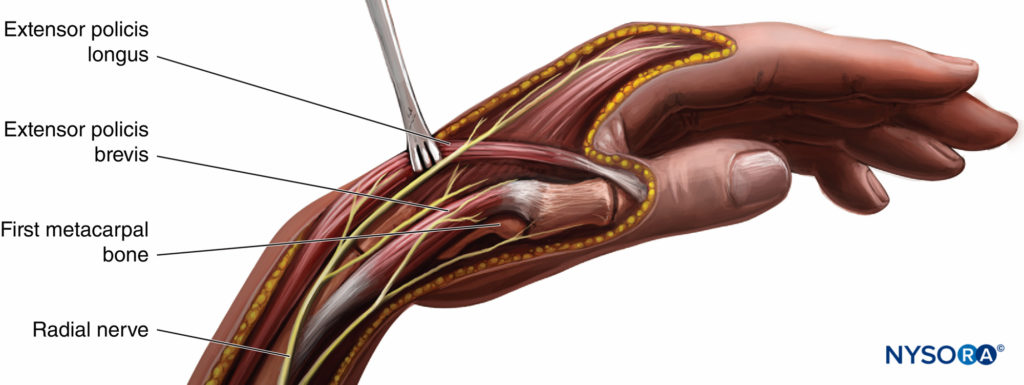
FIGURE 3. Position and course of the radial nerve at the wrist.
ANATOMIC LANDMARKS
The superficial branch of the radial nerve runs along the medial aspect of the brachioradialis muscle (see Figure 3). It then passes between the tendon of the brachioradialis and radius to pierce the fascia on the dorsal aspect. Just above the styloid process of the radius, it gives off digital branches for the dorsal skin of the thumb, index finger, and lateral half of the middle finger. Several of its branches pass superficially over the anatomic “snuff box.” The median nerve is located between the tendons of the palmaris longus and the flexor carpi radialis (Figure 4; see 2). The palmaris longus tendon is usually the more prominent of the two tendons, and the median nerve passes just lateral to it. The ulnar nerve passes between the ulnar artery and tendon of the flexor carpi ulnaris (see Figures 2 and 4). The tendon of the flexor carpi ulnaris is superficial to the ulnar nerve.
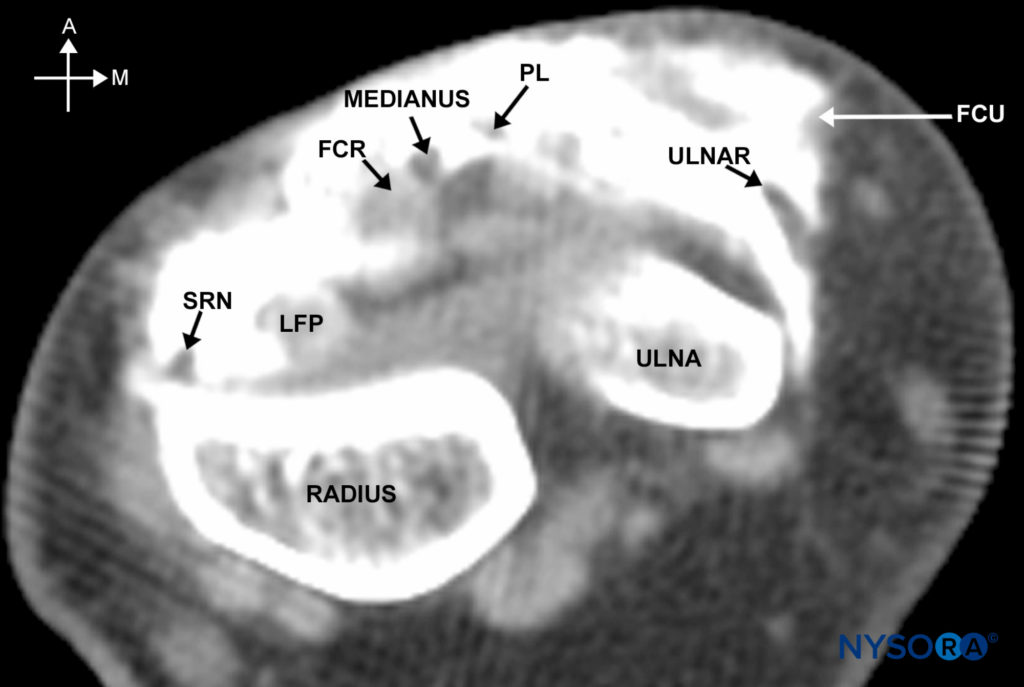
FIGURE 4. Cross-sectional anatomy of the wrist as shown on an MRI scan just above the carpal tunnel. A = anterior, M = medial, SRN = superficial radial nerve, LFP = tendon of the flexor palmaris longus, FCR = flexor carpi radialis, PL = tendon of the palmaris longus, FCU = tendon of the flexor carpi radialis.
EQUIPMENT
A standard regional anesthesia tray is prepared with the following equipment:
- Sterile towels and 4-in. × 4-in. gauze pads
- 10-mL syringes with local anesthetic (LA)
- One 1.5 -in., 25-gauge needle
Learn more about Equipment for Peripheral Nerve Blocks.
TECHNIQUE
The patient is in the supine position with the arm abducted. The wrist should be kept in slight dorsiflexion.
Block of the Radial Nerve
The radial nerve block is essentially a “field block” and requires a more extensive infiltration because of its less predictable anatomic location and division into multiple, smaller cutaneous branches. Five milliliters of LA is injected subcutaneously just above the radial styloid while advancing the needle medially (Figure 5). The infiltration is then extended laterally, using an additional 5 mL of LA.

FIGURE 5. Block of the radial nerve above the head of the radius.
Block of the Dorsal Sensory Branch of the Radial Nerve
The dorsal sensory branch of the radial nerve is blocked by inserting the needle 1 cm proximal to the radial styloid, which is radial to the radial artery (Figure 6). This branch of the radial nerve exits from between the brachioradialis and extensor carpi radialis longus 5–8 cm proximal to the radial styloid. The needle is advanced to the Lister tubercle, and if there are no paresthesias, 5 mL of LA is injected subcutaneously throughout this area.
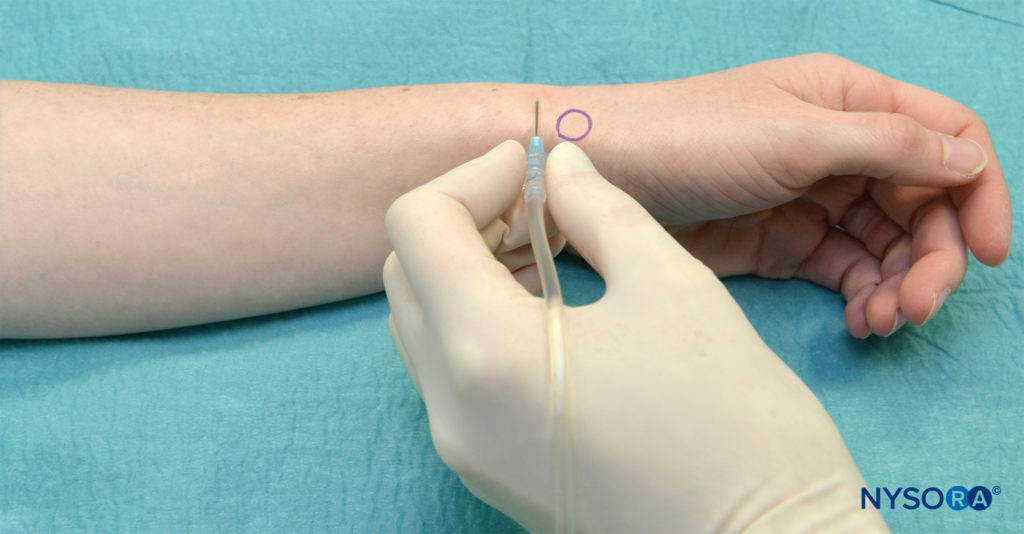
FIGURE 6. Block of the superficial radial nerve
Block of the Ulnar Nerve
The ulnar nerve is anesthetized by inserting the needle under the tendon of the flexor carpi ulnaris muscle close to its distal attachment just above the styloid process of the ulna (Figures 7 and 8; see Figure 4). The needle is advanced 5–10 mm to just past the tendon of the flexor carpi ulnaris. Three to 5 mL of LA solution is injected. Subcutaneous injection of 2–3 mL of local anesthesia just above the tendon of the flexor carpi ulnaris is also advisable in blocking the cutaneous branches of the ulnar nerve, which often extend to the hypothenar area.
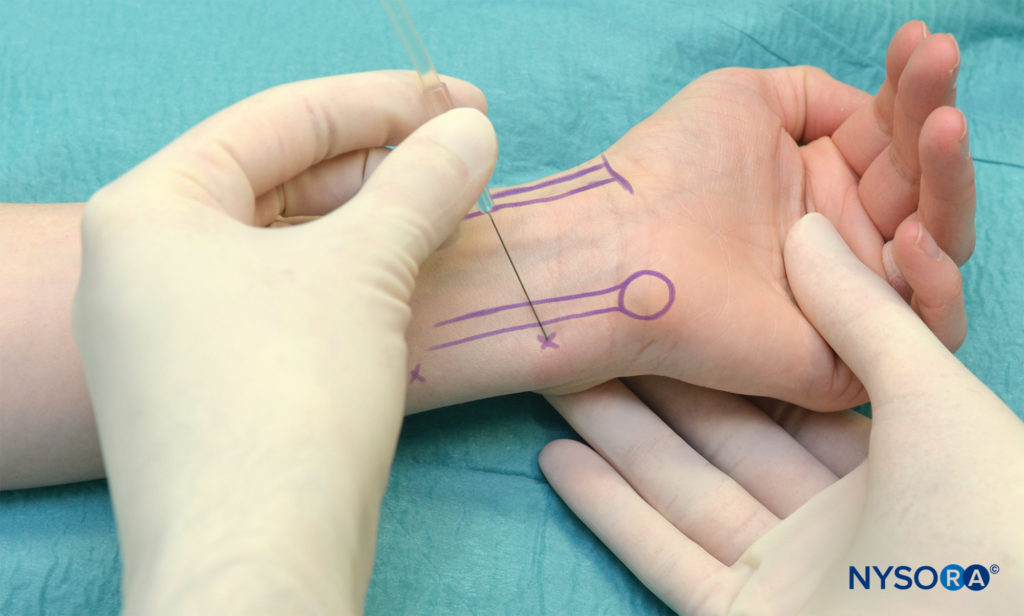
FIGURE 7. Block of the ulnar nerve–the needle is shown inserted just medial to the flexor carpi ulnaris

FIGURE 8. Tendons of the wrist flexors and position of the medianus nerve in relationship to the flexor tendons.
Block of the Dorsal Sensory Branch of the Ulnar Nerve
The dorsal sensory branch of the ulnar nerve is blocked by inserting the needle at the level of the ulnar styloid because it travels from palmar to dorsal in the area of the ulnar styloid (Figure 9). Start the injection at the flexor carpi ulnaris and extend subcutaneously dorsally toward the distal radioulnar joint. Five milliliters of LA is injected subcutaneously throughout the area.

FIGURE 9. Block of the superficial branch of the ulnar nerve.
Block of the Median Nerve
The median nerve is anesthetized by inserting the needle between the tendons of the palmaris longus and flexor carpi radialis (Figures 10 and 11; see Figure 8). The needle is inserted until it pierces the deep fascia. Three to 5 milliliters of LA is injected. Although the piercing of the deep fascia has been described to result in a fascial “click,” it is more reliable to simply insert the needle until it contacts the bone. At that point, the needle is withdrawn 2–3 mm and the LA is injected. Figure 12 demonstrates the spread of the LA after injection of 5 mL using the described technique.
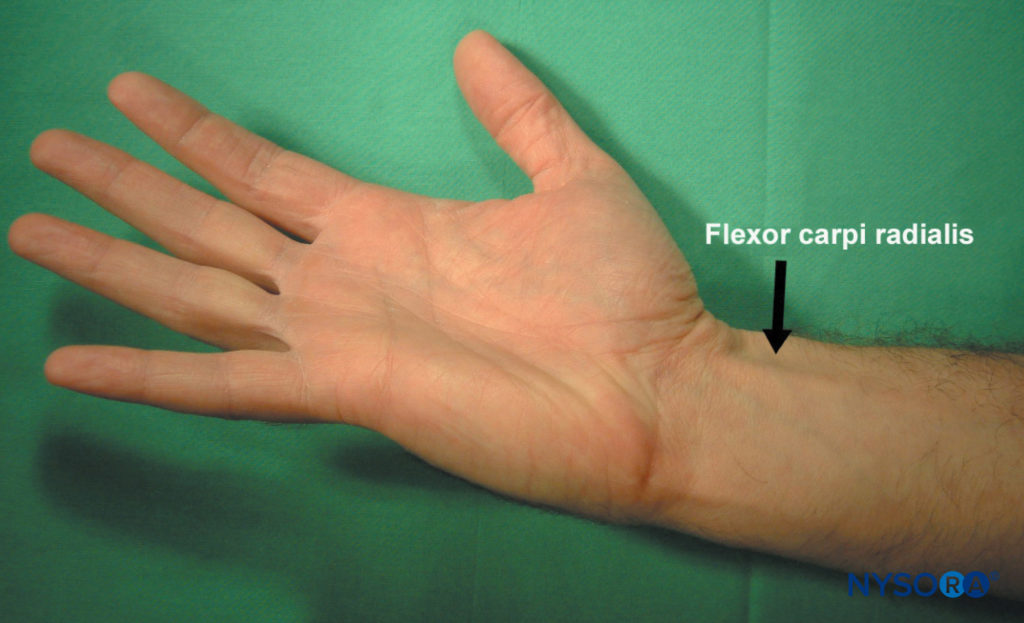
FIGURE 10. A maneuver to accentuate the tendon of the flexor carpi radialis.
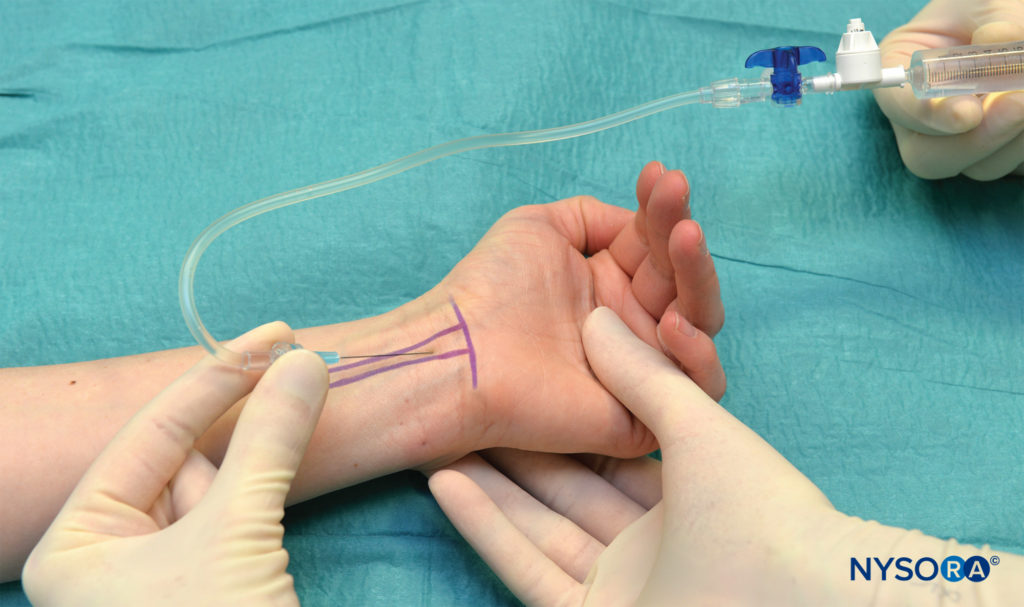
FIGURE 11. Block of the median nerve at the wrist. The needle is shown inserted just medial to the flexor carpi radialis.
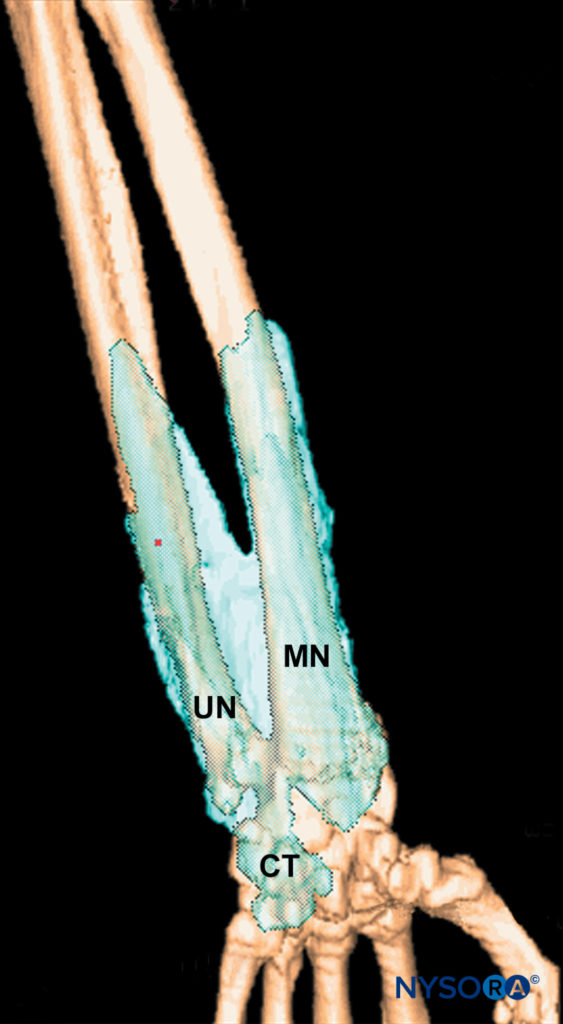
FIGURE 12. Distribution of the dye after wrist block. MN = median nerve, UN = ulnar nerve, CT = carpal tunnel.
NYSORA Tips
- A “fan” technique is recommended to increase the success rate of the median nerve block.
- After the initial injection, the needle is withdrawn back to the skin level, redirected 30 degrees laterally, and advanced again to contact the bone.
- After pulling back 1–2 mm off the bone, an additional 2 mL of LA is injected.
- A similar procedure is repeated with a medial redirection of the needle.
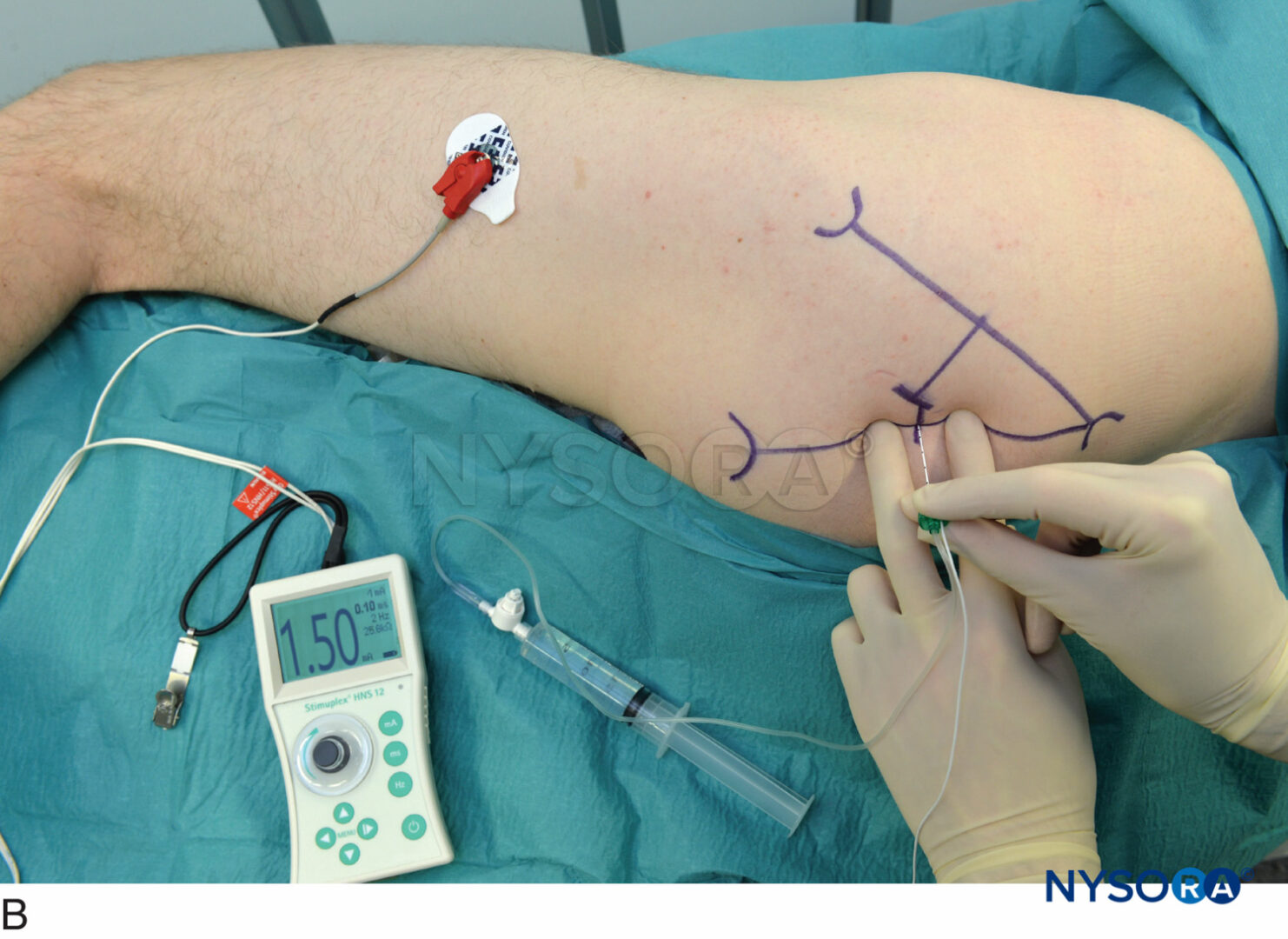
Nerve Stimulation Technique
The median and ulnar nerves can also be blocked at the wrist using a nerve stimulator. These blocks may be used for finger flexor tendon repairs when the surgeon wishes to test their function intraoperatively (the function of the forearm muscles is not affected). The median nerve is found in the carpal tunnel between the palmaris longus and the flexor carpi radialis tendons, and the ulnar nerve is found between the flexor carpi ulnaris and the ulnar artery. Twitches are similar to elbow blocks except for the forearm pronation, which is missing. Two to 3 mL of LA is sufficient to block either nerve.
CHOICE OF LOCAL ANESTHETIC
The choice of the type and concentration of LA for wrist block is based on the desired duration. Lidocaine is the most used anesthetic for wrist block, but bupivacaine can be used safely, also. Table 1 provides onset times and duration for some commonly used LAs. Clean the entire wrist area with a disinfectant solution. Aspirate prior to injection of LA to avoid intravascular injection.
TABLE 1. Onset times and duration for commonly used local anesthetic mixtures.
| Onset (min) | Anesthesia (h) | Analgesia(h) | |
|---|---|---|---|
| 1.5% Mepivacaine (+ HCO3 –) | 15–20 | 2–3 | 3–5 |
| 2% Lidocaine (+ HCO3 –) | 10–20 | 2–5 | 3–8 |
| 0.5% Ropivacaine | 15–30 | 4–8 | 5–12 |
| 0.75% Ropivacaine | 10–15 | 5–10 | 6–24 |
| 0.5% Bupivacaine (or L-bupivacaine) | 15–30 | 5–15 | 6–30 |
BLOCK DYNAMICS AND PERIOPERATIVE MANAGEMENT
This technique is associated with moderate patient discomfort because multiple insertions and subcutaneous injections are required. Appropriate sedation and analgesia, midazolam (2–4 mg) and alfentanil (250–500 mcg), are required to ensure the patient’s comfort. Typical onset time for a wrist block is 10–15 minutes, depending primarily on the concentration of LA used. Sensory anesthesia of the skin develops faster than the motor block. Placement of an Esmarch latex-free bandage or a tourniquet at the level of the wrist is well tolerated and does not require additional block.
NYSORA Tips
- Both nerves lie quite superficially in tight compartments and cannot move away from the needle. Extra caution should, therefore, be used when advancing the needle and injecting LA.
COMPLICATIONS AND HOW TO AVOID THEM
Most common complications after wrist block are residual paresthesias due to an inadvertent intraneural injection. Systemic toxicity is rare because of the distal location of the block (Table 2).
TABLE 2. Complications from wrist block.
| Infection | This should be very rare with the use of an aseptic technique. |
| Hematoma | Avoid multiple needle insertions for superficial blocks. Most superficial blocks can be accomplished with one or two needle insertions. Use 25-gauge needle and avoid puncturing superficial veins. |
| Vascular complications | Do not use epinephrine with wrist and finger blocks. |
| Nerve injury | Do not inject when the patient complains of pain or high pressure on injection is detected. Do not reinject the median and ulnar nerves. |
| Other | Instruct the patient on the care of the insensate extremity. |
This text is a sample of content from the Compendium of Regional Anesthesia on the NYSORA LMS.
NYSORA’s Compendium of Regional Anesthesia is simply the most comprehensive, and practical curriculum on Regional Anesthesia from A to Z, featuring NYSORA’s Premium content. As opposed to textbooks and e-books, the Compendium is continuously updated and features NYSORA’s newest videos, animations, and visual content.
The Compendium is one of several gold-standard educational courses on NYSORA’s Learning System (the NYSORA LMS), and registration to NYSORALMS.com is free. The FULL access to the Compendium, however, is based on an annual subscription, as it requires an army of illustrators, video editors, and an educational team to continue making it the BEST tool for education on everything regional anesthesia. While you can think of the compendium as an ebook on steroids, a quick test drive will give you a real-time feel of how incredible the Compendium really is. Your subscription will transform the way you read about regional anesthesia:
- Learn visually: Everything regional, including spinal, epidural, and nerve block procedures and management protocols
- Review step-by-step techniques instructions for over 60 nerve blocks
- Access NYSORA’s fabled illustrations, animations, and videos (such as Reverse Ultrasound Anatomy)
- Access RA info on any device via the desktop platform and mobile app
- Get real-time updates
- Review infographics for exam preparation (e.g. EDRA)
- Use the Community feed with real case discussions, images and videos are posted and discussed by subscribers and world’s top experts alike.
Even if you do not wish to subscribe to the Compendium, do register to the NYSORA LMS, be the first to know what’s new in regional anesthesia, and get involved in case discussions.
Here’s what the activity feed on NYSORA LMS looks like:
 We are convinced that once you experience the Compendium on the NYSORA LMS, and you’ll never go back to your old books, and your subscription will support keeping NYSORA.com free for the rest of the world.
We are convinced that once you experience the Compendium on the NYSORA LMS, and you’ll never go back to your old books, and your subscription will support keeping NYSORA.com free for the rest of the world.
Additional Reading
- Derkash RS, Weaver JK, Berkeley ME, et al: Office carpal tunnel release with wrist block and wrist tourniquet. Orthopedics 1996;19:589–590.
- Gebhard RE, Al-Samsam T, Greger J, et al: Distal nerve blocks at the wrist for outpatient carpal tunnel surgery offer intraoperative cardiovascular stability and reduce discharge time. Anesth Analg 2002;95:351–355.
- Martinotti R, Berlanda P, Zanlungo M, et al: Peripheral anesthesia techniques in surgery of the arm. Minerva Chir 1999;54:831–833.
- Melone CP Jr, Isani A: Anesthesia for hand injuries. Emerg Med Clin North Am 1985;3:235–243.
- Leversee JH, Bergman JJ: Wrist and digital nerve blocks. J Fam Pract 1981;13:415–421.
- Dushoff IM: Hand surgery under wrist block and local infiltration anesthesia, using an upper arm tourniquet. Plast Reconstr Surg 1973;51: 685–686.
- Vatashsky E, Aronson HB, Wexler MR, et al: Anesthesia in a hand surgery unit. J Hand Surg [Am] 1980;5:495–497.
- Klezl Z, Krejca M, Simcik J: Role of sensory innervation variations for wrist block anesthesia. Arch Med Res 2001;32:155–158.
- Ferrera PC, Chandler R: Anesthesia in the emergency setting: Part I. Hand and foot injuries. Am Fam Physician 1994;50:569–573.
- Agrawal Y, Russon K, Chakrabarti I, Kocheta A. Intra-articular and portal infiltration versus wrist block for analgesia after arthroscopy of the wrist: a prospective RCT. Bone Joint J. 2015; 97-B(9): 1250–1256.
- Delaunay L, Chelly JE: Blocks at the wrist provide effective anesthesia for carpal tunnel release. Can J Anaesth 2001;48:656–660.
- Dupont C, Ciaburro H, Prevost Y, et al: Hand surgery under wrist block and local infiltration anesthesia, using an upper arm tourniquet. Plast Reconstr Surg 1972;50:532–533.
- Paget J: Lectures on Surgical Pathology. Longman, Brown, Green, Longmans/London, 1853.
- Learmonth JR: The principle of decompression in the treatment of certain diseases of peripheral nerves. Surg Clin North Am 1933;13:905–913.
- Dellon AL, Amadio PC: James R. Learmonth: The first peripheral nerve surgeon. J Reconstr Microsurg 2000;16:213–217.
- Phalen GS: Spontaneous compression of the median nerve at the wrist. J Am Med Assoc 1951;145:1128–1133.
- Nystrom A, Lindstrom G, Reiz S, et al: Bupivacaine: A safe local anesthetic for wrist blocks. J Hand Surg [Am] 1989;14:495–498.