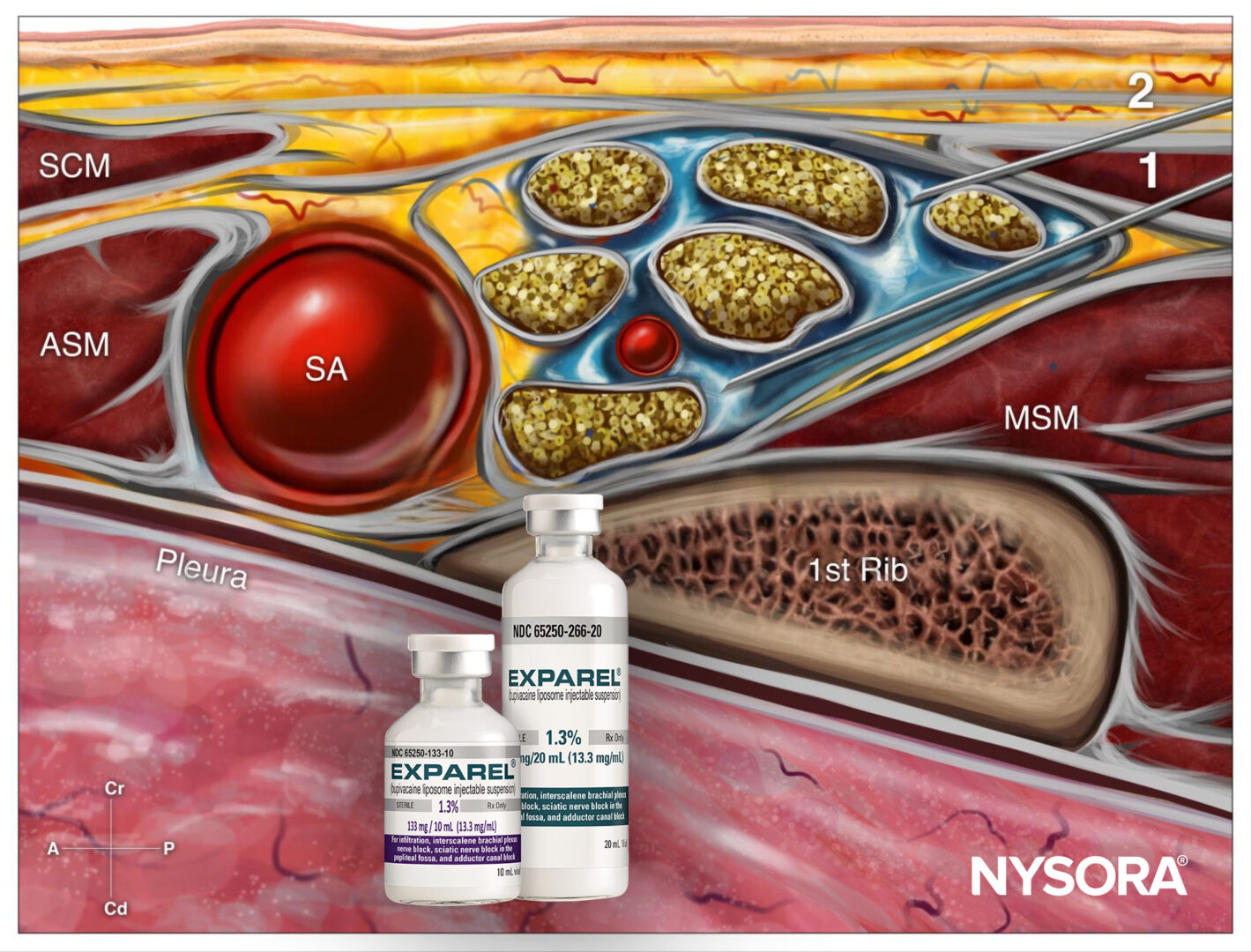
The infraclavicular brachial plexus block targets the brachial plexus at the level of the cords (i.e., lateral, medial, and posterior cords) to provide anesthesia for the arm below the shoulder. Developed as an alternative to supraclavicular blocks, this technique significantly minimizes the risk of complications like pneumothorax. The use of ultrasound further reduces the likelihood of complications, making this approach particularly well-suited for catheter use.
Aguilera et al. 2024 explored the effectiveness of two local anesthetic formulations in ultrasound-guided infraclavicular brachial plexus block (ICBPB) for upper limb surgeries. The trial compared a combination of 0.25% bupivacaine and 1% lidocaine with 0.5% bupivacaine alone, both enhanced with perineural adjuvants.
Key findings
Purpose:
To determine whether 0.5% bupivacaine alone provides longer-lasting motor and sensory blockade compared to a mixture of bupivacaine and lidocaine.
Study design:
- A randomized, double-blind, controlled trial.
- 40 adult patients undergoing upper limb surgery participated.
- Patients were assigned to receive either the bupivacaine-lidocaine mixture or 0.5% bupivacaine.
Outcome measures:
- Primary: Duration of motor block.
Secondary: Sensory block duration, postoperative analgesia duration, and onset time.
Methodology
Procedure:
- All blocks were performed under ultrasound guidance using 35 mL of either local anesthetic solution.
- Perineural adjuvants included epinephrine (5 µg/mL) and dexamethasone (4 mg).
- Sensory and motor blocks were assessed postoperatively.
Assessment scales:
- Motor block: Graded from 0 (no block) to 2 (complete paralysis).
- Sensory block: Graded using pinprick tests from 0 (no block) to 2 (complete anesthesia).
Results
- Block duration:
- Motor block: Lasted significantly longer with 0.5% bupivacaine (28.4 hours) than the mixture (18.9 hours).
- Sensory block: Also longer with 0.5% bupivacaine (29.3 hours) versus the mixture (18.7 hours).
- Postoperative analgesia:
- Patients receiving 0.5% bupivacaine reported extended analgesia duration (38.3 hours) compared to the mixture group (24.3 hours).
- Onset time:
- The bupivacaine-lidocaine mixture achieved a quicker onset (20 minutes) than 0.5% bupivacaine (35 minutes).
- Rebound pain:
- Fewer patients in the 0.5% bupivacaine group (11.1%) experienced severe rebound pain compared to the mixture group (31.6%).
Discussion
Implications for practice:
The findings indicate that 0.5% bupivacaine, combined with perineural dexamethasone and epinephrine, is ideal for prolonging analgesia and block duration, albeit with a delayed onset. This makes it a strong candidate for procedures requiring extended pain relief.
Mechanism:
- Bupivacaine’s high lipophilicity and protein binding likely contribute to its prolonged effect.
- Adding lidocaine shortens onset time but reduces overall block duration due to its medium-acting profile.
Conclusion
This trial highlights the superiority of 0.5% bupivacaine in providing prolonged analgesia and motor-sensory block duration over a bupivacaine-lidocaine mixture despite slower onset. These results support using 0.5% bupivacaine in surgeries requiring extended postoperative pain control, particularly when block onset time is less critical. Further research should explore alternative concentrations and adjuvants for optimizing regional anesthesia techniques.
For more information, refer to the full article in Regional Anesthesia & Pain Medicine.
Aguilera G, Tabilo C, Jara Á, Aliste J. 0.25% bupivacaine-1% lidocaine vs 0.5% bupivacaine for ultrasound-guided infraclavicular brachial plexus block: a randomized controlled trial. Reg Anesth Pain Med. 2024 May 16:rapm-2024-105511.
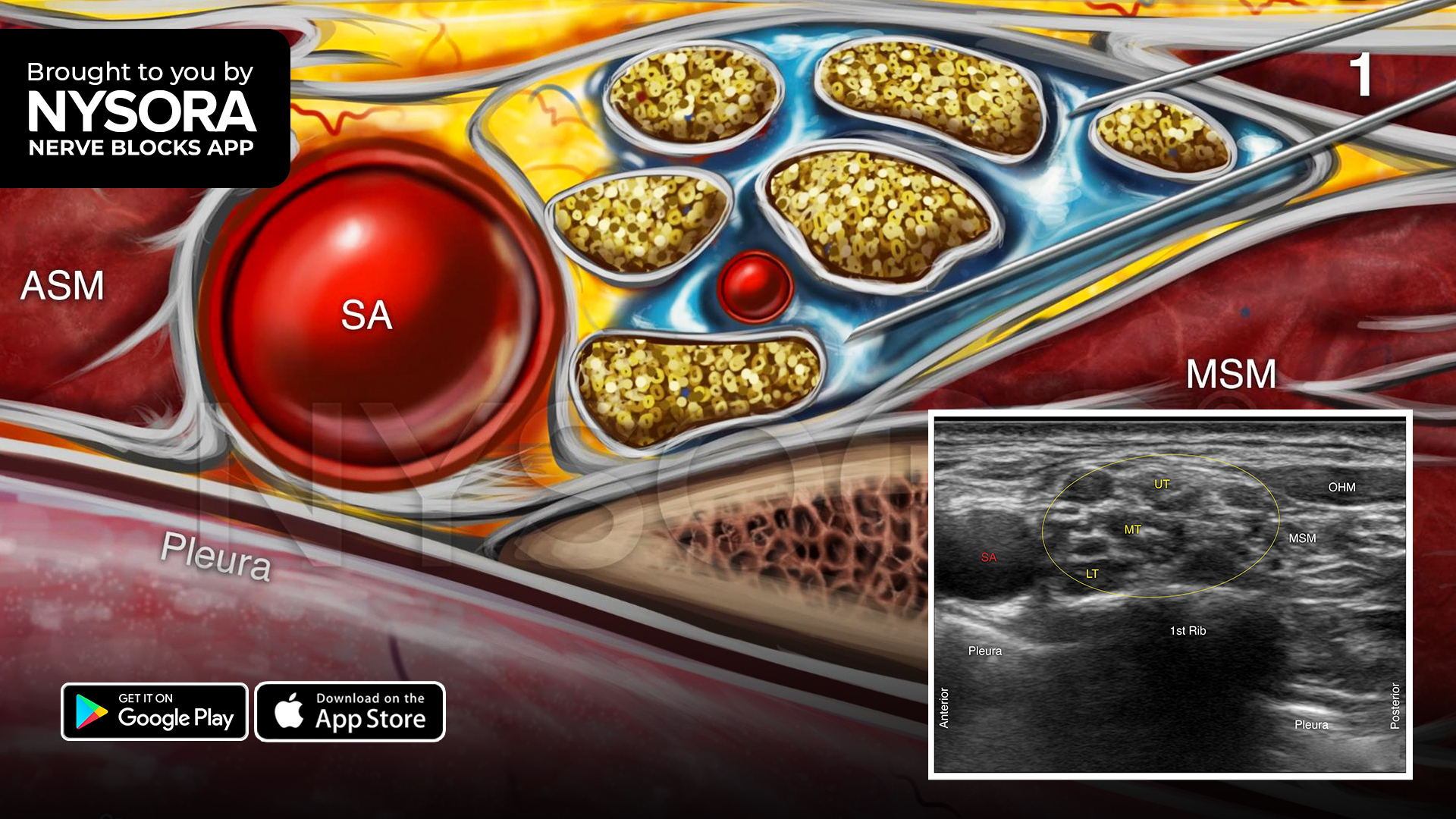
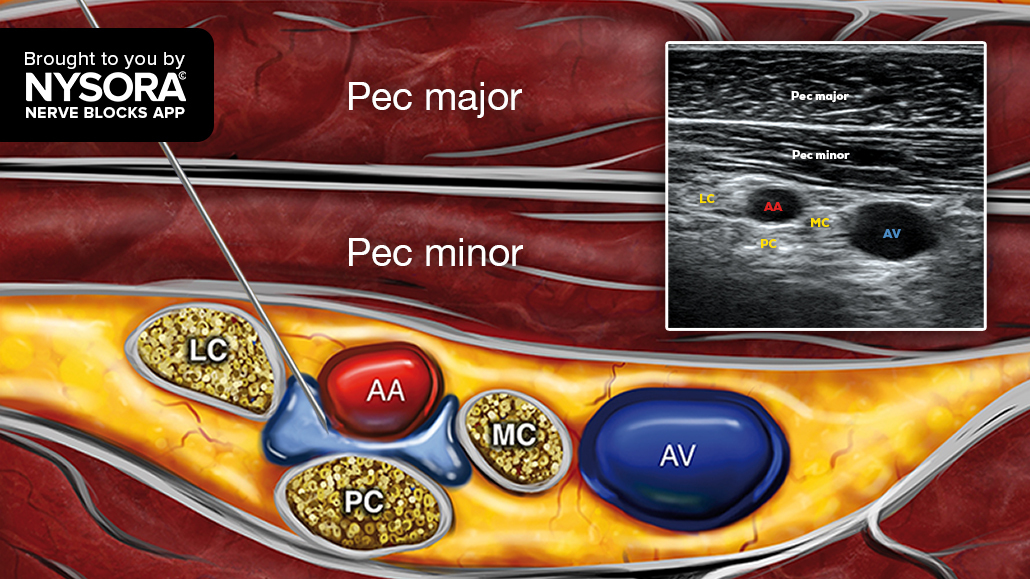
Follow these 3 essential steps for a successful infraclavicular brachial plexus block
- Place the transducer in a sagittal orientation just beneath the clavicle, adjacent to the coracoid process.
- Move the transducer lateral and medial while applying pressure to locate the fascia of the pectoralis minor muscle and the axillary artery (AA) below it at a depth between 3-5 cm.
- Insert the needle in-plane, from cephalad to caudal, behind the AA while avoiding the lateral cord, and inject 20-25 mL of local anesthetic.
Watch the video below to get a better picture of the process and see how the NYSORA Nerve Blocks App brings these instructions to life:
For more tips like these and the complete guide to the 60 most frequently used nerve blocks, download the Nerve Blocks App HERE. Don’t miss the chance to get the bestselling NYSORA Nerve Blocks App also in book format – the perfect study companion with the Nerve Blocks app!