Catherine Vandepitte, Ana M. Lopez, and Hassanin Jalil
FACTS
- Indications: elbow, forearm, and hand surgery
- Transducer position: short axis to arm, just distal to the pectoralis major insertion
- Goal: local anesthetic spread around axillary artery
- Local anesthetic: 15–20 mL
GENERAL CONSIDERATIONS
The axillary brachial plexus block is relatively simple to perform and may be associated with a lower risk of complications compared with interscalene (eg, spinal cord or vertebral artery puncture) and supraclavicular brachial plexus blocks (eg, pneumothorax). In clinical scenarios in which access to the upper parts of the brachial plexus is difficult or impossible (eg, local infection, burns, indwelling venous catheters), the ability to anesthetize the plexus at a more distal level may be important. Although individual nerves can usually be identified this is not absolutely necessary because the deposition of local anesthetic around the axillary artery is sufficient for an effective block.
ULTRASOUND ANATOMY
The structures of interest are superficial (1–3 cm below the skin), and the axillary artery is readily identified within a centimeter of the skin surface on the medial aspect of the proximal arm (Figure 1-A). The artery is accompanied by one or more axillary veins, often located medially to the artery. Importantly, excessive pressure with the transducer during imaging may compress the veins, rendering veins invisible and prone to puncture with the needle. Surrounding the axillary artery, three of the four principal branches of the brachial plexus can be seen: the median (superficial and lateral to the artery), the ulnar (superficial and medial to the artery), and the radial (posterior and lateral or medial to the artery) nerves. The nerves appear as round hyperechoic structures (Figure 1-B). Several authors have reported the anatomical variations of the nerves relative to the axillary artery; Figure 2 illustrates the most common patterns.
Three muscles surround the neurovascular bundle: the biceps (anterior and superficial), the wedge-shaped coracobrachialis (anterior and deep), and the conjoined tendon of the teres major and latissimus dorsi (medial and posterior). The musculocutaneous nerve is located in the fascial layers between the biceps and coracobrachialis muscles, though its location is variable and can be seen within either muscle. It is usually seen as a hypoechoic flattened oval structure with a bright hyperechoic rim. Moving the transducer proximally and distally along the long axis of the arm, the musculocutaneous nerve appears to move toward or away from the neurovascular bundle in the fascial plane between the two muscles. Variations are determined by the position of the musculocutaneous nerve relative to the median nerve and by the position of the ulnar nerve relative to the axillary vein. For additional information see Functional Regional Anesthesia Anatomy.
 Cross-sectional anatomy of the axillary fossa and ultrasound image (B)of the terminal nerves of brachial plexus. The BP is seen scattered around the axillary artery and enclosed")
FIGURE 1. (A) Cross-sectional anatomy of the axillary fossa and ultrasound image (B) of the terminal nerves of brachial plexus. The BP is seen scattered around the axillary artery and enclosed within the adipose tissue compartment containing the axillary artery (AA), and axillary veins (AV). MCN, musculocutaneous nerve. MN, median nerve; RN, radial nerve; UN, ulnar nerve; MACN, medial antebrachial cutaneous nerve; CBM, coracobrachialis muscle.

FIGURE 2. Most common patterns of nerve location around the axillary artery in ultrasound-guided axillary brachial plexus block.
From the Compendium of Regional Anesthesia: Cognitive priming for an axillary brachial plexus block.
DISTRIBUTION OF ANESTHESIA
The axillary brachial plexus block (including the musculocutaneous nerve) results in anesthesia of the upper limb from the mid-arm down to and including the hand. Importantly, the block lends its name from the approach and not from the axillary nerve, which itself is not blocked because it departs from the posterior cord more proximally in the axilla. Therefore, the skin over the deltoid muscle is not anesthetized (Figure 3). With nerve stimulator and landmark-based techniques, the block of the musculocutaneous nerve is often unreliable. However, the musculocutaneous nerve is readily visualized and reliably anesthetized by a separate injection using ultrasound guidance. When required, the medial skin of the upper arm (intercostobrachial nerve, T2) can be blocked by an additional subcutaneous injection just distal to the axilla.

FIGURE 3. Sensory distribution after axillary brachial plexus block.
EQUIPMENT
- Ultrasound machine with linear transducer (8–14 MHz), sterile sleeve, and gel
- Standard nerve block tray
- Syringes with local anesthetic (20 mL)
- 5-cm, 22-gauge, short-bevel, insulated stimulating needle
- Peripheral nerve stimulator
- Opening injection pressure monitoring system
- Sterile gloves
Learn more about Equipment for Peripheral Nerve Blocks
LANDMARKS AND PATIENT POSITIONING
An abduction of the arm to 90 degrees is necessary to allow for transducer placement and needle advancement, (Figure 4). Care should be taken not to over-abduct the arm, as this may cause patient discomfort as well as traction on the brachial plexus, making it theoretically more vulnerable to injury by needle or injection. The pectoralis major muscle is palpated as it inserts onto the humerus, and the transducer is placed on the skin immediately distal to that point, perpendicular to the axis of the arm. The starting point should have the transducer overlying both the biceps and triceps muscles (ie, on the medial aspect of the arm). Sliding the transducer proximally will bring the axillary artery, the conjoint tendon and the terminal branches of the brachial plexus into view, if not readily apparent.
 axillary brachial plexus block. All needle redirections are done through the same needle insertion site.")
FIGURE 4. Patient position and needle insertion for ultrasound-guided (in-plane) axillary brachial plexus block. All needle redirections are done through the same needle insertion site.
GOAL
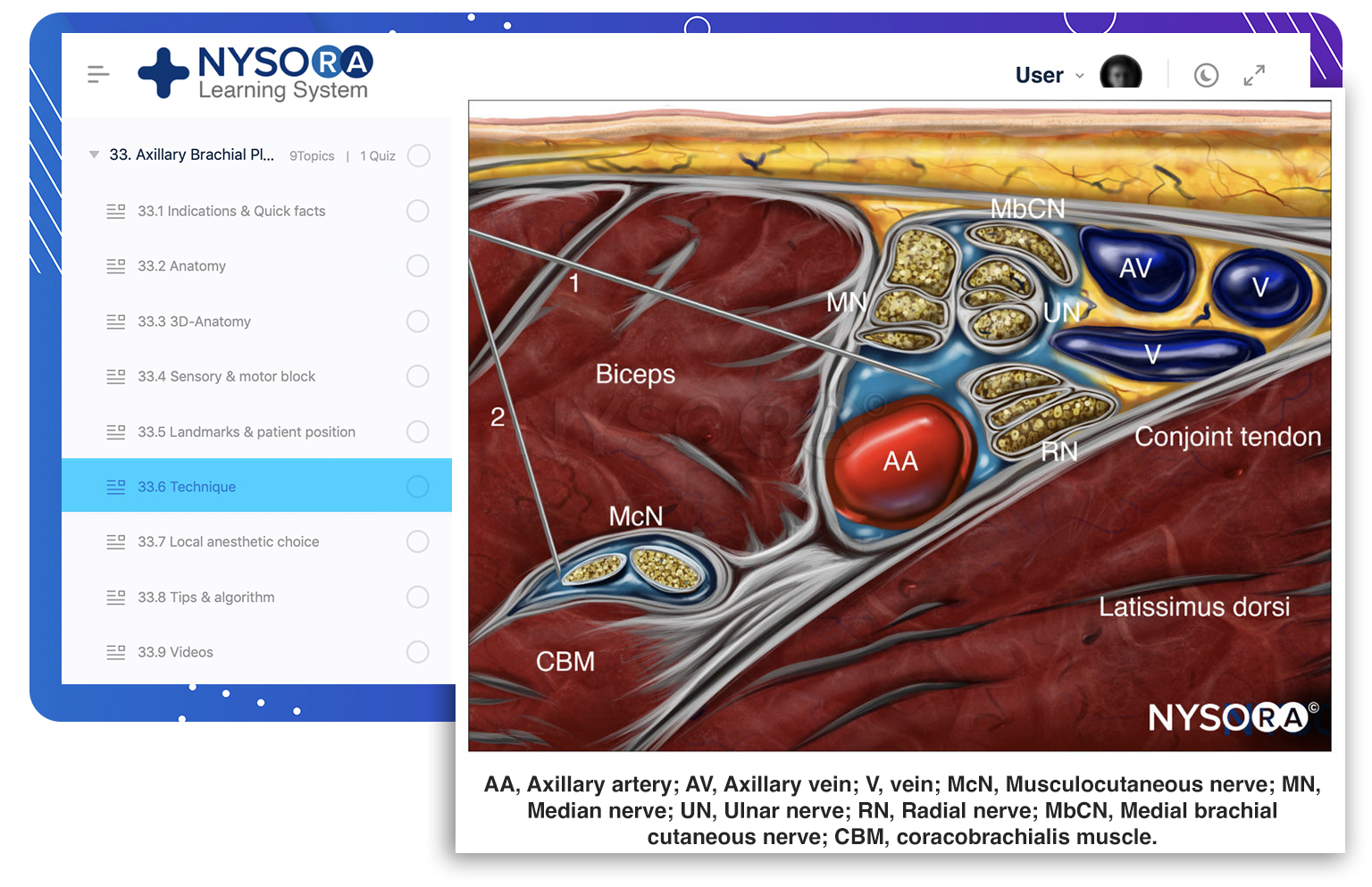
The goal is to deposit local anesthetic around the axillary artery. Typically, two or three injections are required. In addition, an aliquot of local anesthetic should be injected around the musculocutaneous nerve.
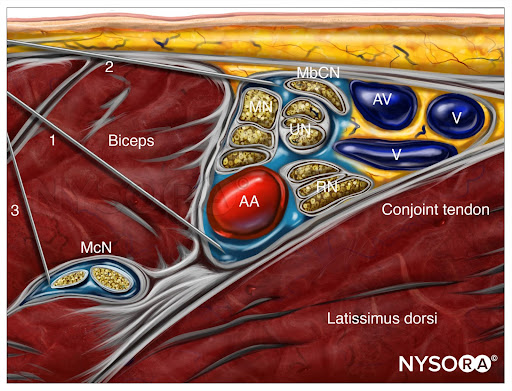
From the Compendium of Regional Anesthesia: Reverse Ultrasound Anatomy for an axillary brachial plexus block with needle insertion in-plane and local anesthetic spread (blue). The figure shows 3 needle injections. AA, axillary artery; AV, axillary vein; McN, musculocutaneous nerve; MN, median nerve; UN, ulnar nerve; RN, radial nerve; MbCN, medial brachial cutaneous nerve.
TECHNIQUE
The skin is disinfected and the transducer is positioned in the short axis orientation to identify the axillary artery about 1–3 cm from the skin surface. Once the artery is identified, an attempt is made to identify the hyperechoic median, ulnar, and radial nerves (Figure 5). However, these may not always be well visualized with ultrasound. Frequently present, an acoustic enhancement artifact deep to the artery is often misinterpreted as the radial nerve. Prescanning should also reveal the position of the musculocutaneous nerve, in the plane between the coracobrachialis and biceps muscles or within either of the muscles (a slight proximal-distal movement of the transducer is often required to bring this nerve into view) (Figure 6).
, ulnar (UN), and radial (RN) nerves are seen scattered around the axillary artery (AA). The musculocutaneous nerve (MCN) is seen between the biceps and coracobrachialis muscle (CBM), away from the rest of the brachial plexus. AV, axillary vein.")
FIGURE 5. The median (MN), ulnar (UN), and radial (RN) nerves are seen scattered around the axillary artery (AA). The musculocutaneous nerve (MCN) is seen between the biceps and coracobrachialis muscle (CBM), away from the rest of the brachial plexus. AV, axillary vein.
 is located few cm away from the axillary artery (AA) between the biceps and the coracobrachialis muscle. The course of the MCN along the upper arm display frequent anatomic variations. Systematic scanning to identify the nerve and a separate injection of local anesthetic are usually required for a successful axillary brachial plexus block.")
FIGURE 6. The musculocutaneous nerve (MCN) is located few cms away from the axillary artery (AA) between the biceps and the coracobrachialis muscle. The course of the MCN along the upper arm display frequent anatomic variations. Systematic scanning to identify the nerve and a separate injection of local anesthetic are usually required for a successful axillary brachial plexus block.
The needle is inserted in-plane from the anterior aspect and directed toward the posterior aspect of the axillary artery (Figure 7). Because nerves and vessels are positioned closely together in the neurovascular bundle by adjacent musculature, advancement of the needle may require careful hydrodissection with a small amount of local anesthetic or other injectates. This technique involves the injection of 0.5–2 mL, indicating the plane in which the needle tip is located. The needle is then carefully advanced stepwise few millimeters at a time. The use of nerve stimulation is recommended to decrease the risk of needle-nerve injury during needle advancement. Local anesthetic should be deposited posterior to the artery first, to avoid displacing the structures of interest deeper and obscuring the nerves, which may occur if injections for the median or ulnar nerves are carried out first.
 and the quality of the image. MCN, musculocutaneous nerve; MN, median nerve; RN, radial nerve; UN, ulnar nerve. AA, axilary vein, AV, axillary vein.")
FIGURE 7. Needle insertions for axillary brachial plexus block. Axillary block can be accomplished by two to four separate injections, depending on the disposition of the nerves around the axillary artery (AA) and the quality of the image. MCN, musculocutaneous nerve; MN, median nerve; RN, radial nerve; UN, ulnar nerve. AA, axilary vein, AV, axillary vein.
The posteriorly located radial nerve is often visualized more clearly once surrounded by local anesthetic. Once 5–7 mL has been administered, the needle is withdrawn almost to the level of the skin, redirected toward the median and ulnar nerves, and a further 7–10 mL is injected in these areas to complete the spread around the nerves. The described sequence of injection is demonstrated in Figure 8.
 and a second one between the ulnar (UN) and radial (RN). The musculocutaneous (MCN)")
FIGURE 8. This image demonstrates the ideal distribution pattern of local anesthetic. In this particular disposition of nerves, a single needle pass superficially to the artery allows for two injections: one for the median (MN) and a second one between the ulnar (UN) and radial (RN). The musculocutaneous (MCN) requires a separate injection.
An alternative, perivascular approach is to simply inject local anesthetic deep to the artery, at the 6 o’clock position, instead of targeting the three nerves individually. This technique may shorten the duration of the block procedure, but also delay onset time, resulting in no difference in total time from skin puncture to the onset of the surgical block. The last step in the procedure, the needle is withdrawn and redirected toward the musculocutaneous nerve. Once adjacent to the nerve (stimulation will result in elbow flexion), 5–7 mL of local anesthetic is deposited. Occasionally, the musculocutaneous nerve will lie in close proximity to the median nerve, rendering a separate injection unnecessary. In an adult patient, 20 mL of local anesthetic is usually adequate for successful block, although successful blocks have been described with smaller volumes. Adequate spread within the axillary brachial plexus sheath is necessary for success but infrequently seen with a single injection. This is accomplished with two to three redirections and injections of 5-7 mL are usually necessary for a reliable block, as well as a separate injection to block the musculocutaneous nerve.
TIPS
- Frequent aspiration and slow administration of local anesthetic are critical for decreasing the risk of intravascular injection. Cases of systemic toxicity have been reported after apparently straightforward ultrasound-guided axillary brachial plexus blocks.
- If no spread is seen on the ultrasound image despite local anesthetic injection, the tip of the needle may be located in a vein. If this occurs, injection should be halted immediately and the needle is withdrawn slightly. Pressure on the transducer should be eased before reassessing the ultrasound image for the presence of vascular structures.
- Anatomic variations in the position of the musculocutaneous nerve have been described. In 16% of cases, the musculocutaneous nerve splits off of the median nerve distally to the axilla. In this case, a separate injection is not needed to block the musculocutaneous nerve as it will be blocked by the local anesthetic injected around the median nerve.
CONTINUOUS ULTRASOUND-GUIDED AXILLARY BLOCK
The indwelling axillary catheter is a useful technique for analgesia and sympathetic block. The goal of the continuous axillary block is to place the catheter within the vicinity of the branches of the brachial plexus (ie, within the “sheath” of the brachial plexus). The procedure is similar to that previously described in Ultrasound-Guided Interscalene Brachial Plexus. The needle is typically inserted in-plane from the anterior to posterior direction, just as in the single-injection technique). After an initial injection of local anesthetic to confirm proper needle tip position posterior to the axillary artery, the catheter is inserted 3–5 cm beyond the needle tip. Injection is then repeated through the catheter to document adequate spread of local anesthetic, wrapping the axillary artery. Alternatively, the axillary artery can be visualized in the longitudinal view with the catheter being inserted in the longitudinal plane alongside the axillary artery. The longitudinal approach requires a significantly greater degree of ultrasonographic skill; no data suggesting that one approach is more effective than the other currently exist.
Continue reading: Axillary Brachial Plexus Block – Landmarks and Nerve Stimulator Technique
Supplementary video related to this block can be found at Ultrasound-Guided Axillary Brachial Plexus Block Video
This text was a sample of content from the Compendium of Regional Anesthesia on the NYSORA LMS.
NYSORA’s Compendium of Regional Anesthesia is simply the most comprehensive, and practical curriculum on Regional Anesthesia from A to Z, featuring NYSORA’s Premium content. As opposed to textbooks and e-books, the Compendium is continuously updated and features NYSORA’s newest videos, animations, and visual content.
The Compendium is one of several gold-standard educational courses on NYSORA’s Learning System (the NYSORA LMS), and registration to NYSORALMS.com is free. The FULL access to the Compendium, however, is based on an annual subscription, as it requires an army of illustrators, video editors, and an educational team to continue making it the BEST tool for education on everything regional anesthesia. While you can think of the compendium as an ebook on steroids, a quick test drive will give you a real-time feel of how incredible the Compendium really is. Your subscription will transform the way you read about regional anesthesia:
- Learn visually: Everything regional, including spinal, epidural, and nerve block procedures and management protocols
- Review step-by-step techniques instructions for over 60 nerve blocks
- Access NYSORA’s fabled illustrations, animations, and videos (such as Reverse Ultrasound Anatomy)
- Access RA info on any device via the desktop platform and mobile app
- Get real-time updates
- Review infographics for exam preparation (e.g. EDRA)
- Use the Community feed with real case discussions, images and videos are posted and discussed by subscribers and world’s top experts alike.
Even if you do not wish to subscribe to the Compendium, do register to the NYSORA LMS, be the first to know what’s new in regional anesthesia, and get involved in case discussions.
Here’s what the activity feed on NYSORA LMS looks like:
We are convinced that once you experience the Compendium on the NYSORA LMS, and you’ll never go back to your old books, and your subscription will support keeping NYSORA.com free for the rest of the world.
Additional Reading
- SConceição DB, Helayel PE, Carvalho FA, Wollmeister J, Oliveira Filho GR: Imagens ultra-sonográficas do plexo braquial na região axilar [Ultrasound images of the brachial plexus in the axillary region]. Rev Bras Anestesiol 2007;57:684–689.
- Christophe JL, Berthier F, Boillot A, et al: Assessment of topographic brachial plexus nerves variations at the axilla using ultrasonography. Br J Anaesth 2009;103:606–612.
- Ustuner E, Yılmaz A, Özgencil E, Okten F, Turhan SC: Ultrasound anatomy of the brachial plexus nerves in the neurovascular bundle at the axilla in patients undergoing upper-extremity block anesthesia. Skeletal Radiol 2013;42:707–713.
- Silva MG, Sala-Blanch X, Marín R, Espinoza X, Arauz A, Morros C: Bloqueo axilar ecoguiado: variaciones anatómicas de la disposición de los 4 nervios terminales del plexo braquial en relación con la arteria humeral [Ultrasound-guided axillary block: anatomical variations of terminal branches of the brachial plexus in relation to the brachial artery]. Rev Esp Anestesiol Reanim 2014;61:15–20.
- Bernucci F, Gonzalez AP, Finlayson RJ, Tran DQ: A prospective, randomized comparison between perivascular and perineural ultrasound-guided axillary brachial plexus block. Reg Anesth Pain Med 2012;37: 473–477.
- O’Donnell B, Riordan J, Ahmad I, Iohom G: Brief reports: a clinical evaluation of block characteristics using one milliliter 2% lidocaine in ultrasound-guided axillary brachial plexus block. Anesth Analg 2010;111: 808–810.
- Robards C, Clendenen S, Greengrass R: Intravascular injection during ultrasound-guided axillary block: negative aspiration can be misleading. Anesth Analg 2008;107:1754–1755.
- Orebaugh SL, Pennington S: Variant location of the musculocutaneous nerve during axillary nerve block. J Clin Anesth 2006;18:541–544.
- Remerand F, Laulan J, Couvret C, et al: Is the musculocutaneous nerve really in the coracobrachialis muscle when performing an axillary block? An ultrasound study. Anesth Analg 2010;110:1729–1734.
- Aguirre J, Blumenthal S, Borgeat A: Ultrasound guidance and success rates of axillary brachial plexus block—I. Can J Anaesth 2007;54:583.
- Alakkad H, Chin KJ: The importance of good needling technique in ultrasound-guided axillary block. Reg Anesth Pain Med 2013;38:166.
- Aveline C: Ultrasound-guided axillary perivascular approach: efficacy and safety remain to be proved. Reg Anesth Pain Med 2013;38:74.
- Baumgarten RK, Thompson GE: Is ultrasound necessary for routine axillary block? Reg Anesth Pain Med 2006;31:88–89.
- Berthier F, Lepage D, Henry Y, Vuillier F, et al: Anatomical basis for ultrasoundguided regional anaesthesia at the junction of the axilla and the upper arm. Surg Radiol Anat 2010;32:299–304.
- Bigeleisen PE: Nerve puncture and apparent intraneural injection during ultrasound-guided axillary block does not invariably result in neurologic injury. Anesthesiology 2006;105:779–783.
- Bloc S, Mercadal L, Garnier T, Komly B, Leclerc P, Morel B, Ecoffey C, Dhonneur G. Comfort of the patient during axillary blocks placement: a randomized comparison of the neurostimulation and the ultrasound guidance techniques. Eur J Anaesthesiol. 2010 Jul;27(7):628-33. [PubMed:20299995]
- Bruhn J, Fitriyadi D, van Geffen GJ: A slide to the radial nerve during ultrasound-guided axillary block. Reg Anesth Pain Med 2009;34:623; author reply 623–624.
- Campoy L, Bezuidenhout AJ, Gleed RD, et al: Ultrasound-guided approach for axillary brachial plexus, femoral nerve, and sciatic nerve blocks in dogs. Vet Anaesth Analg 2010;37:144–153.
- Casati A, Danelli G, Baciarello M, et al: A prospective, randomized comparison between ultrasound and nerve stimulation guidance for multiple injection axillary brachial plexus block. Anesthesiology 2007;106:992–996.
- Chan VW, Perlas A, McCartney CJ, Brull R, Xu D, Abbas S: Ultrasound guidance improves success rate of axillary brachial plexus block. Can J Anaesth 2007;54:176–182.
- Chin KJ, Alakkad H, Cubillos JE: Single, double or multiple-injection techniques for non-ultrasound guided axillary brachial plexus block in adults undergoing surgery of the lower arm. Cochrane Database Syst Rev 2013;8:CD003842.
- Cho S, Kim YJ, Baik HJ, Kim JH, Woo JH: Comparison of ultrasound-guided axillary brachial plexus block techniques: perineural injection versus single or double perivascular infiltration. Yonsei Med J 2015;56:838–844.
- Cho S, Kim YJ, Kim JH, Baik HJ: Double-injection perivascular ultrasoundguided axillary brachial plexus block according to needle positioning: 12 versus 6 o’clock position of the axillary artery. Korean J Anesthesiol 2014;66:112–119.
- Clendenen SR, Riutort K, Ladlie BL, Robards C, Franco CD, Greengrass RA: Real-time three-dimensional ultrasound-assisted axillary plexus block defines soft tissue planes. Anesth Analg 2009;108:1347–1350.
- Dibiane C, Deruddre S, Zetlaoui PJ: A musculocutaneous nerve variation described during ultrasound-guided axillary nerve block. Reg Anesth Pain Med 2009;34:617–618.
- Dolan J, McKinlay S: Early detection of intravascular injection during ultrasound-guided axillary brachial plexus block. Reg Anesth Pain Med 2009;34:182.
- Dufour E, Laloe PA, Culty T, Fischler M: Ultrasound and neurostimulationguided axillary brachial plexus block for resection of a hemodialysis fistula aneurysm. Anesth Analg 2009;108:1981–1983.
- Errando CL, Pallardo MA, Herranz A, Peiro CM, de Andres JA: Bilateral axillary brachial plexus block guided by multiple nerve stimulation and ultrasound in a multiple trauma patient [in Spanish]. Rev Esp Anestesiol Reanim 2006;53:383–386.
- Ferraro LH, Takeda A, dos Reis Falcão LF, Rezende AH, Sadatsune EJ, Tardelli MA: Determination of the minimum effective volume of 0.5% bupivacaine for ultrasound-guided axillary brachial plexus block. Braz J Anesthesiol 2014;64:49–53.
- Forero CM, Gomez Lora CP, Bayegan D: Undetected intravascular injection during an ultrasound-guided axillary block. Can J Anaesth 2013;60:329–30.
Fregnani JH, Macéa MI, Pereira CS, Barros MD, Macéa JR: Absence of the musculocutaneous nerve: a rare anatomical variation with possible clinical-surgical implications. Sao Paulo Med J 2008;126:288–290. - Frkovic V, Ward C, Preckel B, et al: Influence of arm position on ultrasound visibility of the axillary brachial plexus. Eur J Anaesthesiol 2015;32: 771–780.
- Gelfand HJ, Ouanes JP, Lesley MR, et al: Analgesic efficacy of ultrasound-guided regional anesthesia: meta-analysis. J Clin Anesth 2011;232:90–96.
- González AP, Bernucci F, Pham K, Correa JA, Finlayson RJ, Tran DQ:Minimum effective volume of lidocaine for double-injection ultrasoundguided axillary block. Reg Anesth Pain Med 2013;38:16–20.
- Gray AT: The conjoint tendon of the latissimus dorsi and teres major: an important landmark for ultrasound-guided axillary block. Reg Anesth Pain Med 2009;34:179–180.
- Gray AT, Schafhalter-Zoppoth I: “Bayonet artifact” during ultrasound-guided transarterial axillary block. Anesthesiology 2005;102:1291–1292.
- Hadžic A, Dewaele S, Gandhi K, Santos A: Volume and dose of local anesthetic necessary to block the axillary brachial plexus using ultrasound guidance. Anesthesiology 2009;111:8–9.
- Harper GK, Stafford MA, Hill DA: Minimum volume of local anaesthetic required to surround each of the constituent nerves of the axillary brachial plexus, using ultrasound guidance: a pilot study. Br J Anaesth 2010;104:633–636.
- Imasogie N, Ganapathy S, Singh S, Armstrong K, Armstrong P: A prospective, randomized, double-blind comparison of ultrasound-guided axillary brachial plexus blocks using 2 versus 4 injections. Anesth Analg 2010;110:1222–1226.
- Jung MJ, Byun HY, Lee CH, Moon SW, Oh MK, Shin H: Medial antebrachial cutaneous nerve injury after brachial plexus block: two case reports. Ann Rehabil Med 2013;37:913–918.
- Kjelstrup T, Courivaud F, Klaastad Ø, Breivik H, Hol PK: High-resolution MRI demonstrates detailed anatomy of the axillary brachial plexus. A pilot study. Acta Anaesthesiol Scand 2012;56:914–919.
- Kjelstrup T, Hol PK, Courivaud F, Smith HJ, Røkkum M, Klaastad Ø: MRI of axillary brachial plexus blocks: a randomised controlled study. Eur J Anaesthesiol 2014;31:611–619.
- Kokkalis ZT, Mavrogenis AF, Saranteas T, Stavropoulos NA, Anagnostopoulou S: Ultrasound-guided anterior axilla musculocutaneous nerve block. Radiol Med 2014;119:135–141.
- Liu FC, Liou JT, Tsai YF, et al: Efficacy of ultrasound-guided axillary brachial plexus block: a comparative study with nerve stimulator-guided method. Chang Gung Med J 2005;28:396–402.
- Lo N, Brull R, Perlas A, et al: Evolution of ultrasound guided axillary brachial plexus block: retrospective analysis of 662 blocks. Can J Anaesth 2008;55:408–413.
- López-Morales S, Moreno-Martín A, Leal del Ojo JD, Rodriguez-Huertas F: Bloqueo axilar ecoguiado frente a bloqueo infraclavicular ecoguiado para la cirugía de miembro superior [Ultrasound-guided axillary block versus ultrasound-guided infraclavicular block for upper extremity surgery]. Rev Esp Anestesiol Reanim 2013;60:313–319.
- Luyet C, Constantinescu M, Waltenspül M, Luginbühl M, Vögelin E: Transition from nerve stimulator to sonographically guided axillary brachial plexus anesthesia in hand surgery: block quality and patient satisfaction during the transition period. J Ultrasound Med 2013;32: 779–786.
- Luyet C, Schüpfer G, Wipfli M, Greif R, Luginbühl M, Eichenberger U: Different learning curves for axillary brachial plexus block: ultrasound guidance versus nerve stimulation. Anesthesiol Res Pract 2010;2010:309462.
- Mannion S, Capdevila X: Ultrasound guidance and success rates of axillary brachial plexus block—II. Can J Anaesth 2007;54:584.
- Marhofer P, Eichenberger U, Stockli S, et al: Ultrasonographic guided axillary plexus blocks with low volumes of local anaesthetics: a crossover volunteer study. Anaesthesia 2010;65:266–271.
- Morros C, Pérez-Cuenca MD, Sala-Blanch X, Cedó F: Bloqueo axilar del plexo braquial guiado por ecografía. Curva de aprendizaje y resultados [Ultrasound-guided axillary brachial plexus block: learning curve and results]. Rev Esp Anestesiol Reanim 2011;58:74–79.
- Morros C, Perez-Cuenca MD, Sala-Blanch X, Cedo F: Contribution of ultrasound guidance to the performance of the axillary brachial plexus block with multiple nerve stimulation [in Spanish]. Rev Esp Anestesiol Reanim 2009;56:69–74.
- O’Donnell BD, Iohom G. An estimation of the minimum effective anesthetic volume of 2% lidocaine in ultrasound-guided axillary brachial plexus block. Anesthesiology 2009;111:25–29.
- O’Donnell BD, Ryan H, O’Sullivan O, Iohom G: Ultrasound-guided axillary brachial plexus block with 20 milliliters local anesthetic mixture versus general anesthesia for upper limb trauma surgery: an observer-blinded, prospective, randomized, controlled trial. Anesth Analg 2009;109: 279–283.
- O’Sullivan O, Aboulafia A, Iohom G, O’Donnell BD, Shorten GD: Proactive error analysis of ultrasound-guided axillary brachial plexus block performance. Reg Anesth Pain Med 2011;36:502–507.
- O’Sullivan O, Shorten GD, Aboulafia A: Determinants of learning ultrasound-guided axillary brachial plexus block. Clin Teach 2011;8:236–240.
- Orebaugh SL, Williams BA, Vallejo M, Kentor ML: Adverse outcomes associated with stimulator-based peripheral nerve blocks with versus without ultrasound visualization. Reg Anesth Pain Med 2009;34:251–255.
- Perlas A, Chan VW, Simons M: Brachial plexus examination and localization using ultrasound and electrical stimulation: a volunteer study. Anesthesiology 2003;99:429–435.
- Perlas A, Niazi A, McCartney C, Chan V, Xu D, Abbas S: The sensitivity of motor response to nerve stimulation and paresthesia for nerve localization as evaluated by ultrasound. Reg Anesth Pain Med 2006;31:445–450.
- Porter JM, McCartney CJ, Chan VW: Needle placement and injection posterior to the axillary artery may predict successful infraclavicular brachial plexus block: a report of three cases. Can J Anaesth 2005;52: 69–73.
- Ranganath A, Srinivasan KK, Iohom G: Ultrasound guided axillary brachial plexus block. Med Ultrason 2014;16:246–251.
- Russon K, Blanco R: Accidental intraneural injection into the musculocutaneous nerve visualized with ultrasound. Anesth Analg 2007;105:1504–1505.
- Russon K, Pickworth T, Harrop-Griffiths W. Upper limb blocks. Anaesthesia 2010;65(Suppl 1):48–56.
- Saranteas T, Anagnostopoulou S, Kostopanagiotou G: Ultrasound imaging in anaesthesia: which is the optimal anatomic point to block the radial nerve in the axilla? Anaesth Intensive Care 2009;37:328–329.
- Satapathy AR, Coventry DM: Axillary brachial plexus block. Anesthesiol Res Pract 2011;2011:173796.
- Schoenmakers KP, Wegener JT, Stienstra R: Effect of local anesthetic volume (15 vs 40 mL) on the duration of ultrasound-guided single shot axillary brachial plexus block: a prospective randomized, observer-blinded trial. Reg Anesth Pain Med 2012;37:242–247.
- Schwemmer U, Schleppers A, Markus C, Kredel M, Kirschner S, Roewer N: Operative management in axillary brachial plexus blocks: comparison of ultrasound and nerve stimulation [in German]. Anaesthesist 2006;55: 451–456.
- Sites BD, Beach ML, Spence BC, et al: Ultrasound guidance improves the success rate of a perivascular axillary plexus block. Acta Anaesthesiol Scand 2006;50:678–684.
- Spence BC, Sites BD, Beach ML: Ultrasound-guided musculocutaneous nerve block: a description of a novel technique. Reg Anesth Pain Med 2005; 30:198–201.
- Strub B, Sonderegger J, Von Campe A, Grünert J, Osterwalder JJ: What benefits does ultrasound-guided axillary block for brachial plexus anaesthesia offer over the conventional blind approach in hand surgery? J Hand Surg Eur Vol 2011;36:778–786.
- Sultan SF, Iohom G, Saunders J, Shorten G: A clinical assessment tool for ultrasound-guided axillary brachial plexus block. Acta Anaesthesiol Scand 2012;56:616–623.
- Takeda A, Ferraro LH, Rezende AH, Sadatsune EJ, Falcão LF, Tardelli MA: Minimum effective concentration of bupivacaine for axillary brachial plexus block guided by ultrasound. Braz J Anesthesiol 2015;65:163–169.
- Tedore TR, YaDeau JT, Maalouf DB, et al: Comparison of the transarterial axillary block and the ultrasound-guided infraclavicular block for upper extremity surgery: a prospective randomized trial. Reg Anesth Pain Med 2009;34:361–365.
- Tran DQ, Clemente A, Tran DQ, Finlayson RJ: A comparison between ultrasound-guided infraclavicular block using the “double bubble” sign and neurostimulation-guided axillary block. Anesth Analg 2008;107: 1075–1078.
- Tran DQ, Pham K, Dugani S, Finlayson RJ: A prospective, randomized comparison between double-, triple-, and quadruple-injection ultrasound-guided axillary brachial plexus block. Reg Anesth Pain Med 2012;37: 248–253.
- Tran DQ, Russo G, Muñoz L, Zaouter C, Finlayson RJ: A prospective, randomized comparison between ultrasound-guided supraclavicular, infraclavicular, and axillary brachial plexus blocks. Reg Anesth Pain Med 2009;34:366–371.
- Veneziano GC, Rao VK, Orebaugh SL: Recognition of local anesthetic maldistribution in axillary brachial plexus block guided by ultrasound and nerve stimulation. J Clin Anesth 2012;24:141–144.
- Wong DM, Gledhill S, Thomas R, Barrington MJ: Sonographic location of the radial nerve confirmed by nerve stimulation during axillary brachial plexus block. Reg Anesth Pain Med 2009;34:503–507.
- Wong MH, George A, Varma M: Ultrasound-guided perivascular axillary brachial plexus block: not so simple. Reg Anesth Pain Med 2013;38:167.
- Yang ZX, Pho RW, Kour AK, Pereira BP: The musculocutaneous nerve and its branches to the biceps and brachialis muscles. J Hand Surg Am 1995;20: 671–675.
- Zetlaoui PJ, Labbe JP, Benhamou D: Ultrasound guidance for axillary plexus block does not prevent intravascular injection. Anesthesiology 2008;108:761.