The anatomy of the adductor canal and its role in the multimodal analgesic regimen for knee arthroplasty is a frequently discussed topic during the NYSORA workshops. Here are some answers to the questions regarding the best injection site and identifying the anatomical boundaries between the femoral triangle and the adductor canal.
Three related, but different techniques are the “subsartorial blocks”: the subsartorial saphenous nerve block, the adductor canal block, and the femoral triangle block.
- The subsartorial saphenous nerve block (SSNB) aims to anesthetize the medial aspect of the leg, ankle, and midfoot. It is commonly performed as an adjunct to the sciatic nerve block for lower leg surgery.
- The adductor canal block (ACB) is similar to the subsartorial saphenous nerve block, as the injection occurs in the same anatomical space. The difference is that in the adductor canal block, larger volumes of local anesthetic are used. ACB was introduced as an alternative to the femoral nerve block to avoid quadriceps paresis after knee surgery.
- The femoral triangle block (FTB) consists of an injection of the local anesthetic proximal to the adductor canal. The goal is to anesthetize additional terminal branches of the femoral nerve for better analgesia after knee surgery. The drawback is more motor weakness of the quadriceps muscle.
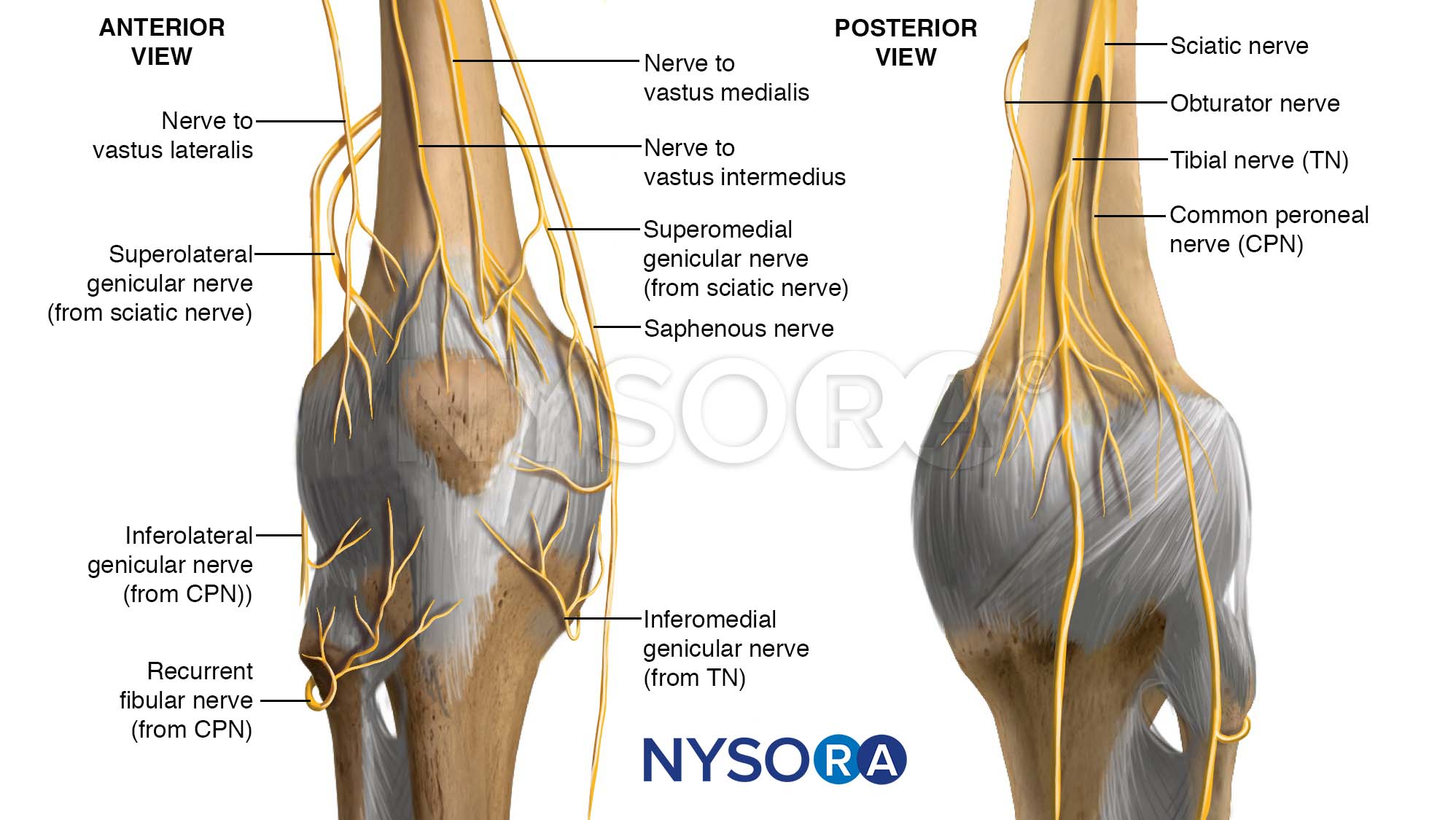
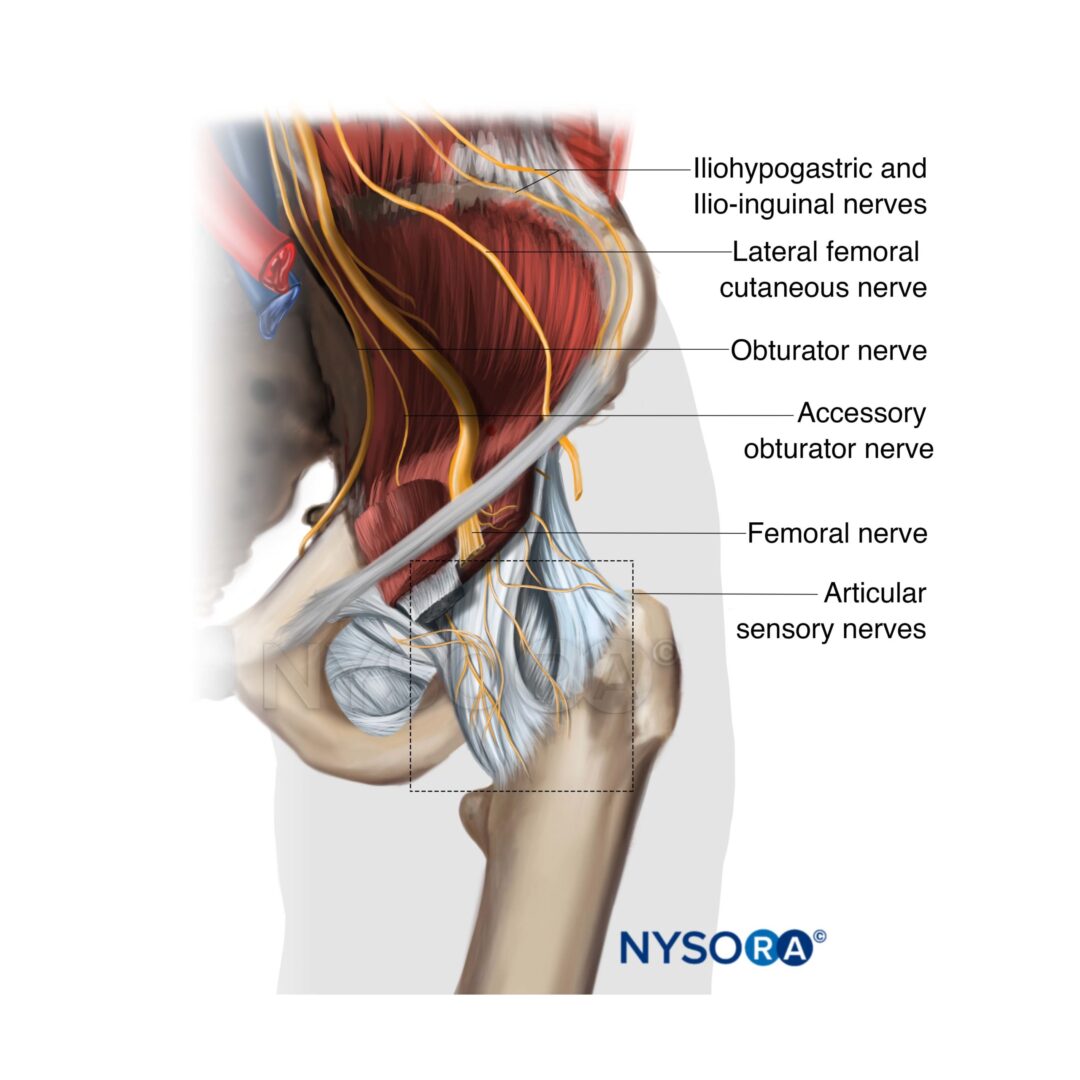
Although the analgesic efficacy of the adductor canal technique is well documented, the ideal injection level remains a matter of debate among the practitioners. Anatomical studies indicate that the adductor canal in addition to the saphenous nerve, also contains the medial femoral cutaneous nerve, branches from the nerve to the vastus medialis, and articular branches from the obturator nerve. These additional nerve branches contribute to the innervation of the anteromedial aspect of the knee.
There are two important factors to consider when performing this block:
1) Injection level (proximal or distal)
2) The volume of local anesthetic
If the block is performed proximally (femoral triangle) or with a large volume of local anesthetic, the spread proximally will reach more branches of the femoral nerve, resulting in better analgesia, but greater quadriceps weakness. An adductor canal injection spares the strength of the quadriceps muscle. However, it also confers more limited analgesia.
Identify the adductor canal in 3 STEPS
- Place the transducer transversely over the medial part of the proximal leg and identify the femoral artery and vein.
- Slide the transducer posteriorly to visualize the border of the sartorius and adductor longus muscle.
- Slide the transducer proximally-distally to identify the point where the medial border of the sartorius muscle meets the medial border of the adductor longus muscle as demonstrated in the video below. This triangle-shaped border is the limit between the apex of the femoral triangle and the proximal end of the adductor canal.
TIP: An injection proximal to this point (3) will be in the femoral triangle, whereas an injection distal to it will occur in the adductor canal.