Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe cerebral palsy
- Recognize the symptoms and signs of cerebral palsy
- Outline the anticipated challenges for airway management in patients with cerebral palsy
- Identify common intraoperative complications associated with cerebral palsy
Definition and mechanisms
- Cerebral palsy (CP) is a group of permanent neurodevelopmental disorders that affects an individual’s muscle tone, motor functions, movement, and posture
- CP is attributed to non-progressive disturbances that occur in the developing fetal or infant brain
- CP is the most common motor disability in childhood
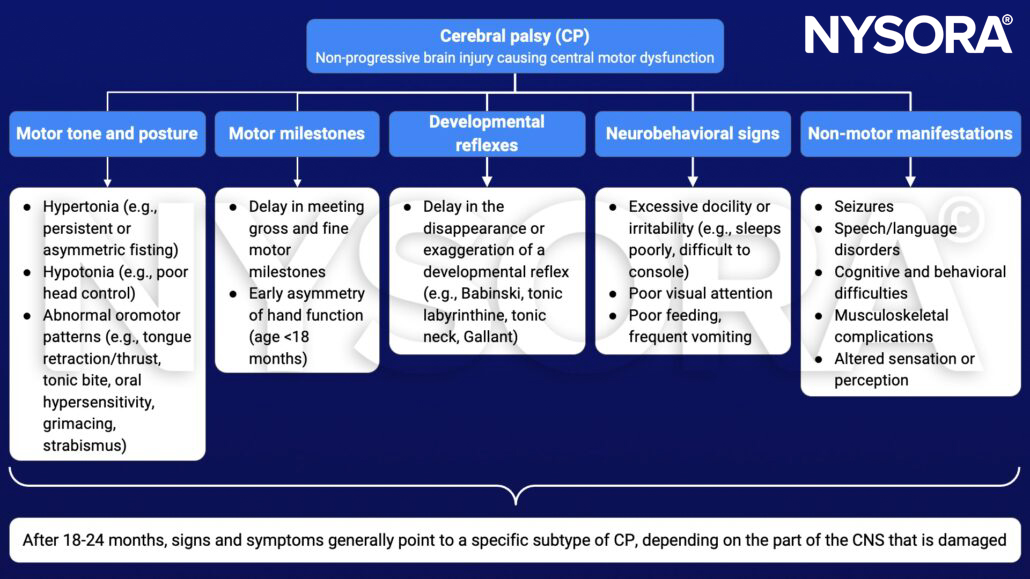
Signs and symptoms
- Signs and symptoms vary among people
- CP can affect the whole body or might be limited primarily to one or two limbs, or one side of the body
- Symptoms get more noticeable over the first few years of life, but underlying problems do not worsen over time
Movement and coordination
- Stiff muscles and exaggerated reflexes (spasticity)
- Variations in muscle tone (too stiff or floppy)
- Stiff muscles with normal reflexes (rigidity)
- Lack of balance and muscle coordination (ataxia)
- Tremors or jerky involuntary movements
- Favoring one side of the body (e.g., only reaching with one hand or dragging a leg while crawling)
- Difficulty walking (e.g., walking on toes, crouched gait, scissors-like gait with knees crossing, wide gait, or asymmetrical gait)
- Difficulty with fine motor skills
Speech and eating
- Delays in speech development
- Difficulty speaking
- Difficulty with sucking, chewing, or eating
- Excessive drooling or problems with swallowing
Development
- Delays in reaching motor skills milestones (babies with CP do not roll over, sit, crawl, or walk as early as other children of their age)
- Learning disability
- Intellectual disability
- Delayed growth (smaller size than expected)
Other problems
- Epilepsy
- Difficulty hearing
- Problems with vision and abnormal eye movements
- Abnormal touch or pain sensations
- Bladder and bowel problems (e.g., constipation and urinary incontinence)
- Mental health conditions (e.g., emotional disorders and behavioral problems)
Risk factors
Congenital CP (80%)
- Fetal pathogenic factors
- Vascular maldevelopments
- Congenital genetic/metabolic disorders
- Microcephaly
- Fetal trauma
- Neonatal asphyxia in the peripartum period (6%)
- Low birth weight (<2.5 kg)
- Prematurity (<32 weeks)
- Low Apgar score
- Multiple births
- Prenatal “TORCH” infections (toxoplasmosis, rubella, cytomegalovirus, and herpes)
- Maternal pathogenic factors
- Breech presentation
- Pre-eclampsia
- Peripartum hemorrhage
- Maternal hyperthyroidism
- Fetal alcohol syndrome
Acquired CP (20%) → develops during the first 2 years of life
- Intracerebral hemorrhage
- Viral encephalitis
- Bacterial meningitis
- Hyperbilirubinemia (kernicterus)
- Head injury
- Neonatal seizures
Complications
Muscle weakness, muscle spasticity, and coordination problems may contribute to complications during childhood or adulthood
- Contracture: Muscle tissue shortening due to severe muscle tightening as a result of spasticity → can inhibit bone growth, cause bones to bend, and result in joint deformities, dislocation, or partial dislocation (e.g., hip dislocation, scoliosis)
- Malnutrition: Swallowing or feeding problems limit the infant to get enough nutrition → impair growth and weaken bones
- Mental health conditions: Depression and behavioral problems
- Cardiopulmonary disease
- Increased risk of aspiration pneumonitis and subsequent chronic lung scarring due to swallowing difficulties, esophageal dysmotility, abnormal lower esophageal sphincter tone, and spinal deformity → gastroesophageal reflux disease (GERD)
- Decreased immunity, poor nutrition, respiratory muscle hypotonia, and a weak cough in conjunction with GERD make patients more susceptible to recurrent chest infections, exacerbating the underlying chronic lung disease
- Long-term truncal muscle spasticity can lead to scoliosis, restrictive lung defects, pulmonary hypertension, and ultimately cor pulmonale and respiratory failure
- Osteoarthritis: Pressure on joints or abnormal alignment of joints from muscle spasticity may lead to the early onset of osteoarthritis
- Osteoporosis: Fractures due to low bone density resulting from lack of mobility, inadequate nutrition, and anti-epileptic drug use
- Other complications: Sleep disorders, chronic pain, skin breakdown, intestinal problems, and issues with oral health
Pathophysiology

Treatment
Treatment is focused on
- Improving posture and mobility by reducing spasticity, muscle spasms, and contractures
- Symptomatic relief of the associated medical problems (e.g., epilepsy, GERD, chest infections)
Combination therapies are more successful than single-treatment protocols: Physiotherapy, psychological counseling, occupational, speech, and behavioral therapy combined with
- Antispastic medications (e.g., baclofen)
- Neuromuscular denervation techniques (e.g., botulinum toxin injections, radiofrequency ablation of dorsal horn ganglia, and dorsal rhizotomy)
- Surgery (e.g., tenotomies, arthrodeses, osteotomies tendon transfer/lengthening, and multisegmental spinal fusion procedures)
Management
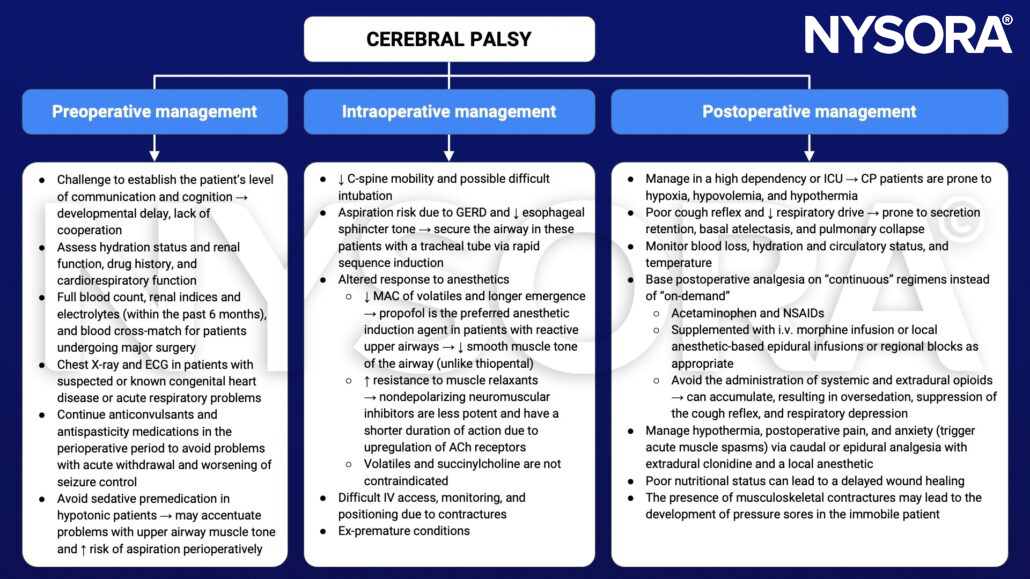
Keep in mind
- CP describes a spectrum of movement and posture disorders resulting from pathological injury to the developing fetal or infant brain
- Commonly associated comorbidities include dehydration, malnutrition, epilepsy, GERD, and impaired lung function
- Frequently encountered perioperative problems include difficulties with patient positioning and vascular access
- Regional analgesic techniques to reduce postoperative pain, muscle spasms, and respiratory complications are beneficial
Suggested reading
- Prosser DP, Sharma N. Cerebral palsy and anaesthesia. Continuing Education in Anaesthesia Critical Care & Pain. 2010;10(3):72-76.
- Miller B, Rondeau B. Anesthetic Considerations In Patients With Cerebral Palsy. [Updated 2022 Jun 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572057/
Clinical updates
Nielsen et al. (Regional Anesthesia & Pain Medicine, 2017) demonstrate that ultrasound-guided obturator nerve block reliably anesthetizes the obturator nerve and its hip articular branches, supporting its use in managing painful hip adductor spasticity. This technique is particularly relevant in children with cerebral palsy, where targeted obturator nerve blockade can reduce spasticity, improve perioperative comfort, and complement orthopedic surgical management.
- Read more about this topic HERE.