Jerry D. Vloka, Ann-Sofie Smeets, Tony Tsai, and Cedric Bouts
INTRODUCTION
Cervical plexus anesthesia was developed early in the 20th century with two main approaches being used. In 1912, Kappis described a posterior approach to the cervical and brachial plexus, which attempted to block the nerves at their point of emergence from the vertebral column. The posterior approach was advocated because the vertebral artery and vein lie anterior to the plexus. However, the needle must pass through the extensor muscles of the neck which causes considerable discomfort, and the long path of the needle is more hazardous. Consequently, this technique is not recommended as a routine for cervical or brachial plexus block.
In 1914, Heidenhein described the lateral approach, which has formed the basis for subsequent techniques of anesthetizing the cervical plexus. Victor Pauchet also described a lateral approach to blocking the cervical plexus in 1920 and recommended it over the posterior approach. Winnie revisited the lateral approach to the cervical plexus block in 1975, and described a simplified, single-injection technique. The lateral approach is currently the more commonly used approach and will be described in this chapter.
INDICATIONS AND CONTRAINDICATIONS
Deep and superficial cervical plexus blocks can be used in a variety of surgical procedures, including superficial surgery on the neck and shoulders and thyroid surgery. Its use is most common in carotid endarterectomy, in which an awake patient self-monitors to ensure adequate cerebral blood flow during cross-clamping of the carotid artery (Figure 1). Since the description of the first carotid endarterectomy in 1954 by Eastcott, the number of these operations has been growing annually. Regional anesthesia is a viable anesthetic choice for carotid surgery, although debate continues whether it improves patient outcomes. The largest randomized trial to date on this topic (GALA trial) showed no difference in 30-day stroke or mortality rates, a conclusion that has been supported by a recent meta-analysis.
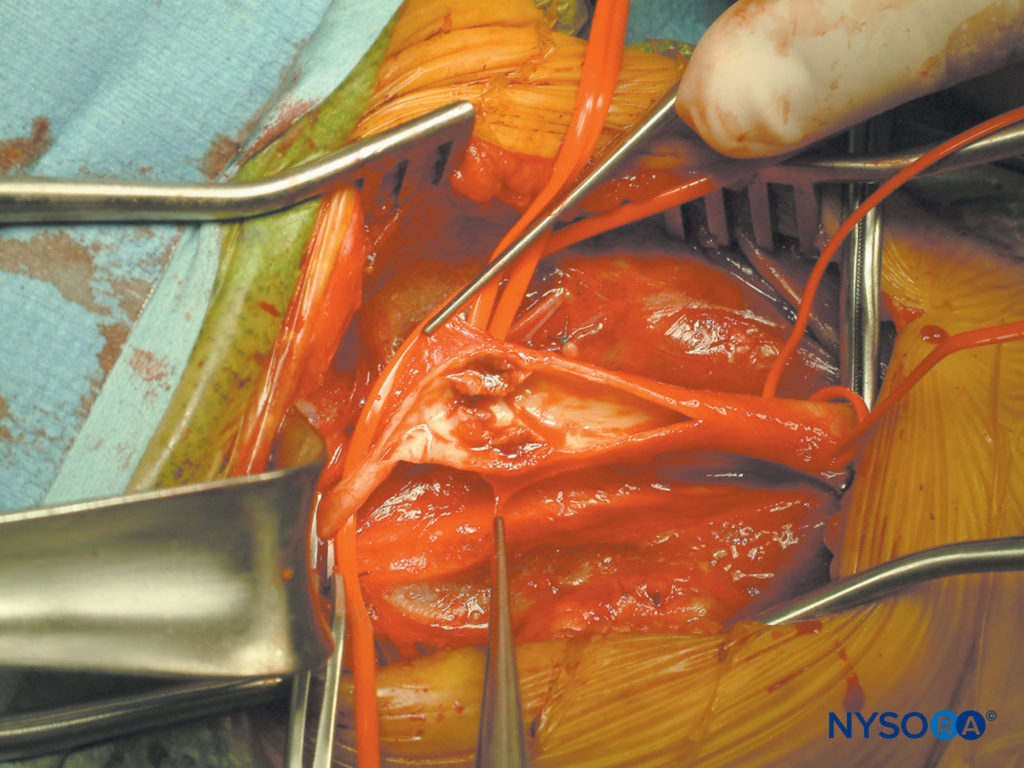
Figure 1. Carotid endarterectomy. The image shows open, cross-clamped carotid artery and a plaque inside its wall.
The superficial cervical plexus block can be used for many superficial surgeries in the neck area, including lymph node dissection, excision of thyroglossal or branchial cleft cysts, carotid endarterectomy, and vascular access surgery.
Comparisons of superficial vs deep cervical plexus blocks for carotid endarterectomy have either shown equivalence or favored the superficial block due to the lower risk of complications.
Although both the deep and superficial cervical plexus blocks can be performed separately, they have been used by some also in combination for anesthesia and postoperative analgesia for head and neck surgery.
Contraindications to performing a cervical plexus block include patient refusal, local infection, and previous surgery or radiation therapy to the neck. Likewise, due to the risk of phrenic nerve paresis, the deep cervical plexus block is relatively contraindicated in patients with contralateral phrenic nerve palsy and significant pulmonary compromise.
FUNCTIONAL ANATOMY OF DEEP CERVICAL PLEXUS block
The cervical plexus is formed by the anterior divisions of the four upper cervical nerves (Figure 2). The plexus is situated on the anterior surface of the four upper cervical vertebrae, resting on the levator anguli scapulae and scalenus medius muscles, and is covered by the sternocleidomastoid muscle.
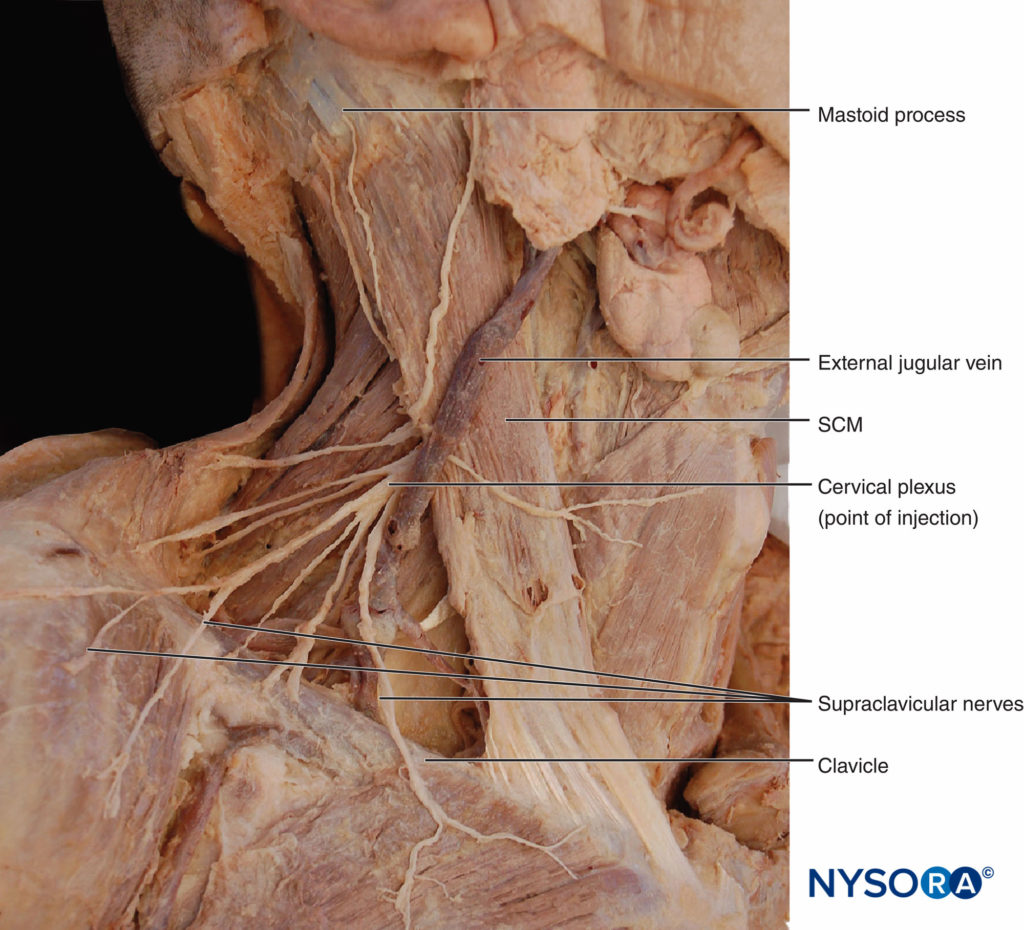
Figure 2. Anatomy of the cervical plexus.
The dorsal and ventral roots combine to form spinal nerves as they exit through the intervertebral foramen. The first cervical root is primarily a motor nerve and is of little interest for locoregional anesthesia. The anterior rami of the second through fourth cervical nerves form the cervical plexus. The branches of the superficial cervical plexus innervate the skin and superficial structures of the head, neck, and shoulder (Figure 3). The branches of the deep cervical plexus innervate the deeper structures of the neck, including the muscles of the anterior neck and the diaphragm, which is innervated by the phrenic nerve. The third and fourth cervical nerves send a branch to the spinal accessory nerve, or directly into the deep surface of the trapezius to supply sensory fibers to this muscle. The fourth cervical nerve may send a branch downward to join the fifth cervical nerve and participate in the formation of the brachial plexus.
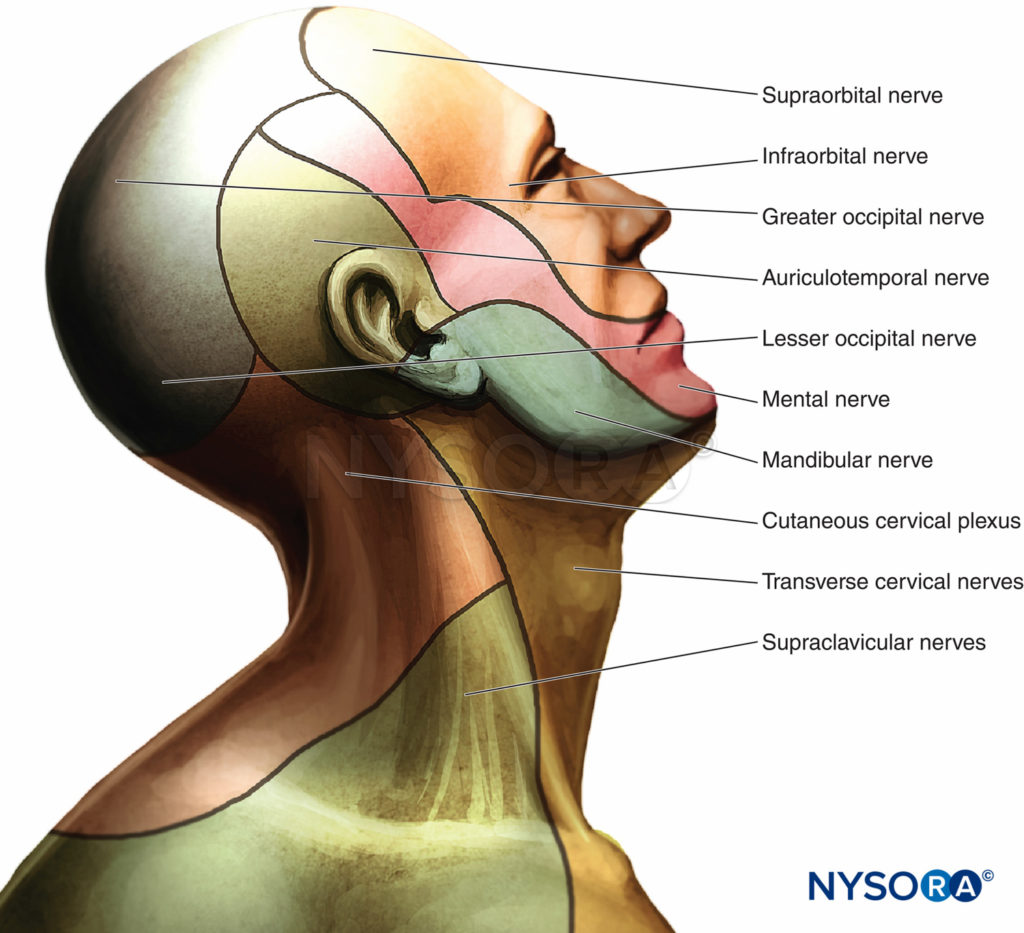
Figure 3.. Innervation of the head and neck
The cutaneous innervation of both the deep and superficial cervical plexus blocks includes the skin of the anterolateral neck and the anteauricular and retroauricular areas (Figure 3). To read more about the cervical plexus distribution, see Functional Regional Anesthesia Anatomy.
Anatomic Landmarks
The following three landmarks for a deep cervical plexus block are identified and marked (Figure 4):
- Mastoid process
- Chassaignac tubercle (the transverse process of the sixth cervical vertebra)
- The posterior border of the sternocleidomastoid muscle
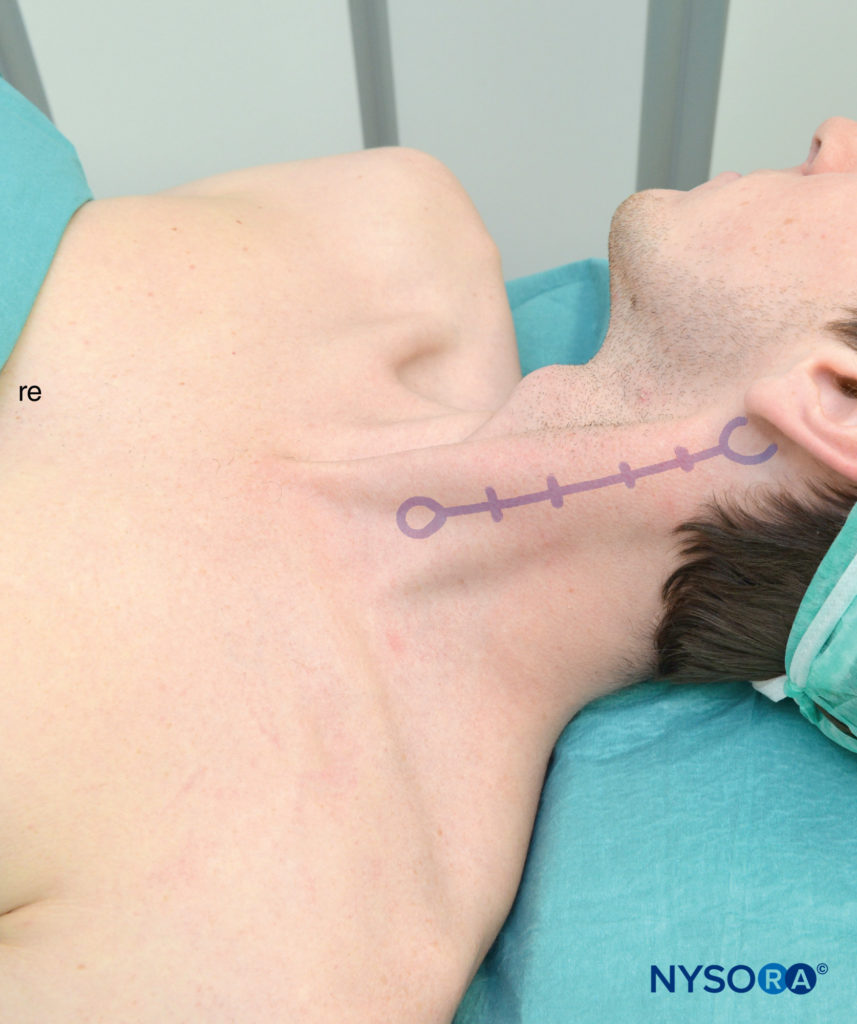
Figure 4. Anatomic landmarks for the cervical plexus. Shown are estimates of the transverse processes C2-C3-C4-C5-C6.
To estimate the line of needle insertion that overlies the transverse processes, the mastoid process (MP) and the Chassaignac tubercle, which is the transverse process of the sixth cervical vertebra (C6), are identified and marked (Figure 5).
Figure 5. Palpation of the transverse process of C6.
The transverse process of C6 is usually easily palpated behind the clavicular head of the sternocleidomastoid muscle at the level just below the cricoid cartilage (Figure 6). Next, a line is drawn connecting the MP to the Chassaignac tubercle. Position the palpating hand just behind the posterior border of the sternocleidomastoid muscle. Once this line is drawn, label the insertion sites over the C2, C3, and C4, which are respectively located on the MP–C6 line 2 cm, 4 cm, and 6 cm, respectively, caudal to the mastoid process.

Figure 6. Palpation of the mastoid process.
It is also possible to perform a single injection at the C3 level, which is considered safe and effective.
- The distances specified for spacing along the transverse processes at various levels are estimates at best.
- Once two neighboring transverse processes are identified, the spacing between the other transverse processes follows a similar pattern.
NYSORA Tips
Choice of Local Anesthetic
A deep cervical plexus block requires 3–5 mL of local anesthetic per level to ensure a reliable block. Except perhaps with patients with significant respiratory disease who rely on their phrenic nerve to adequately ventilate, most patients benefit from the use of a long-acting local anesthetic. Table 1 shows commonly used local anesthetics with onset and duration of anesthesia and analgesia for deep cervical plexus blocks. Ropivacaine 0.5% provides a good quality block of longer duration, and it is one of most common choices for carotid endarterectomy surgery.
TABLE 1. Commonly used local anesthetics for deep cervical plexus blocks.
| Onset (min) | Anesthesia (h) | Analgesia (h) | |
|---|---|---|---|
| 1.5% Mepivacaine (+ HCO3 – + epinephrine) | 10–15 | 2.0–2.5 | 3–6 |
| 2% Lidocaine (+ HCO3 – + epinephrine) | 10–15 | 2–3 | 3–6 |
| 0.5% Ropivacaine | 10–20 | 3–4 | 4–10 |
| 0.25% Bupivacaine (+ epinephrine) | 10–20 | 3–4 | 4–10 |
Equipment
A standard regional anesthesia tray is prepared with the following equipment:
- Sterile towels and 4-in. × 4-in. gauze pads
- 20-mL syringe(s) with local anesthetic
- Sterile gloves and marking pen
- One 1.5 -in., 25-gauge needle for skin infiltration
- A 1.5 -in.-long, 22-gauge, short-beveled needle
Learn more about Equipment for Regional Anesthesia.
Technique
After cleaning the skin with an antiseptic solution, local anesthetic is infiltrated subcutaneously along the line estimating the position of the transverse processes. The needle should contact the posterior tubercle of the transverse process where the spinal nerves at the individual levels are located just in front of the transverse process.
The block needle is connected to a syringe with local anesthetic via flexible tubing. The block needle is inserted between the palpating fingers and advanced at an angle perpendicular to the skin. A slight caudal orientation of the needle prevents the inadvertent insertion of the needle toward the cervical spinal cord. The needle should never be oriented cephalad. The needle is advanced slowly until the transverse process is contacted (Figure 7). At this point, the needle is withdrawn 1–2 mm and stabilized for injection of 4 mL of local anesthetic per level after negative aspiration for blood. The block needle is then removed, and the procedure is repeated at consecutive levels.
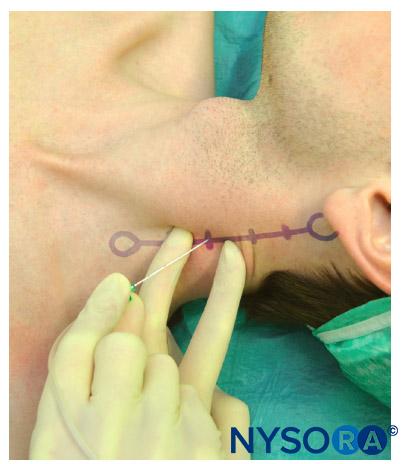
Figure 7. Needle insertion to block a single cervical level during deep cervical block.
NYSORA Tips
- The transverse process is typically contacted at a depth of 1–2 cm in most patients.
- Never advance the needle beyond 2.5 cm due to the risk of spinal cord injury.
- Paresthesia is often elicited in proximity to the transverse process but should not be relied on as the successful needle placement because of its nonspecific radiating pattern
Block Dynamics and Perioperative Management
Although the placement of deep cervical block may be uncomfortable for the patient, excessive sedation should be avoided. During surgery, airway management may be difficult due to the close proximity of the surgical field. Surgeries like carotid endarterectomy require that the patient be cooperative for intraoperative neurologic assessment. Excessive sedation and the consequent lack of patient cooperation can lead to restlessness and patient movement intraoperatively.
The onset time for this block is 10–15 min. The first sign of onset is decreased sensation in the distribution of the respective components of the cervical plexus. It should be noted that due to the complex arrangement of the neuronal coverage of the various layers in the neck area as well as cross coverage from the contralateral side, the anesthesia achieved with cervical plexus block is often incomplete, and its use often requires a knowledgeable surgeon who is skilled in supplementing the block with local anesthetic as necessary.
NYSORA Tips
- Carotid surgery also requires block of the glossopharyngeal nerve branches, which is easily accomplished intraoperatively by injecting the local anesthetic inside the carotid artery sheath.
FUNCTIONAL ANATOMY OF SUPERFICIAL CERVICAL PLEXUS block
The superficial cervical plexus innervates the skin of the anterolateral neck (see Figure 3). The terminal branches emerge as four distinct nerves from the posterior border of the sternocleidomastoid muscle. The lesser occipital nerve is usually a direct branch from the main stem of the second cervical nerve. The larger remaining part of this stem then unites with a part of the third cervical nerve to form a trunk that gives rise to the greater auricular and transverse cervical nerves. Another part of the third cervical nerve runs downward to unite with a major part of the fourth cervical nerve to form a supraclavicular trunk, which then divides into the three groups of supraclavicular nerves.
Anatomic Landmarks
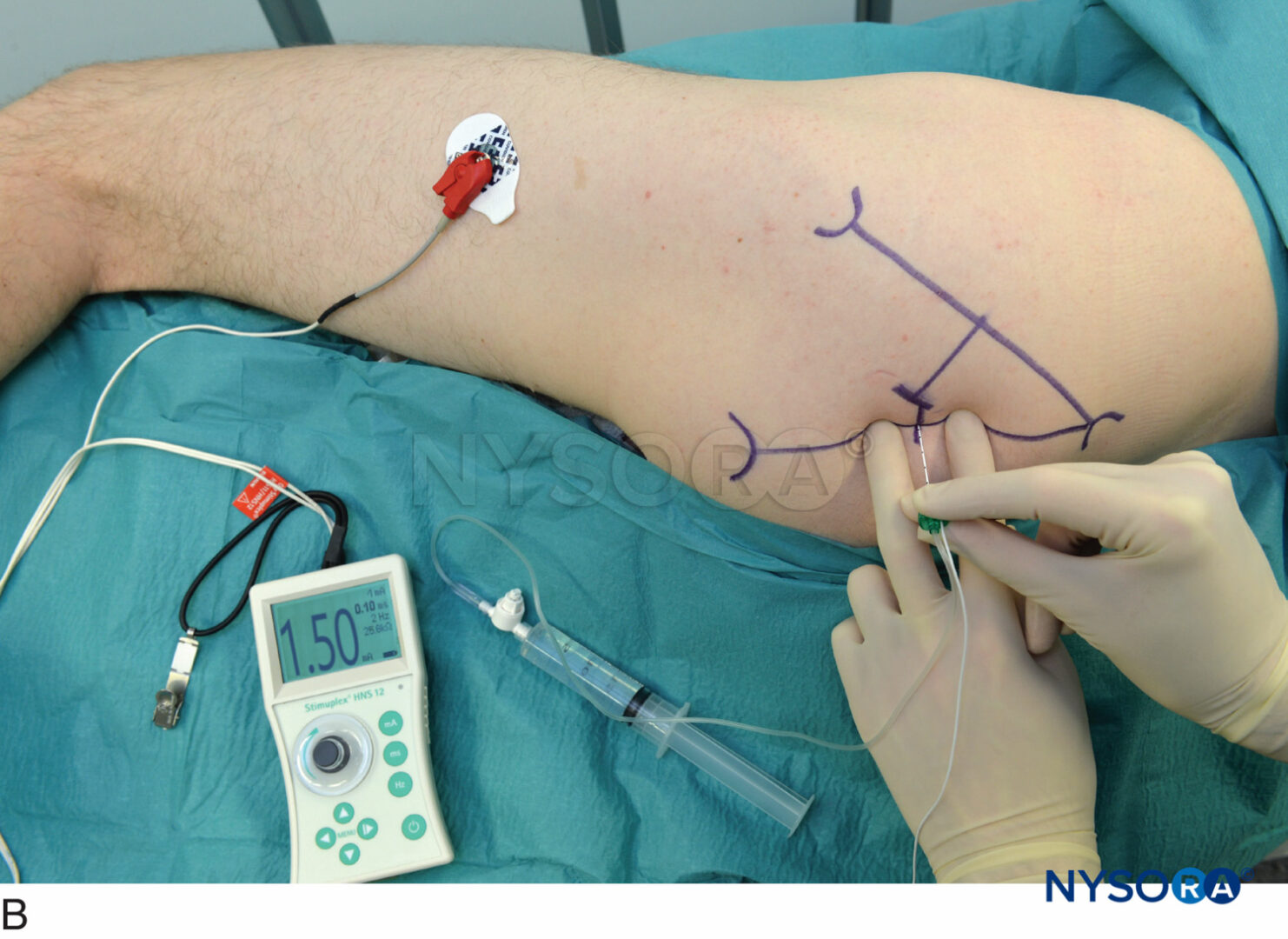
A line extending from the mastoid process to C6 is drawn as described above (Figure 8). The site of needle insertion is marked at the midpoint of this line. This is where the branches of the superficial cervical plexus emerge from behind the posterior border of the sternocleidomastoid muscle.
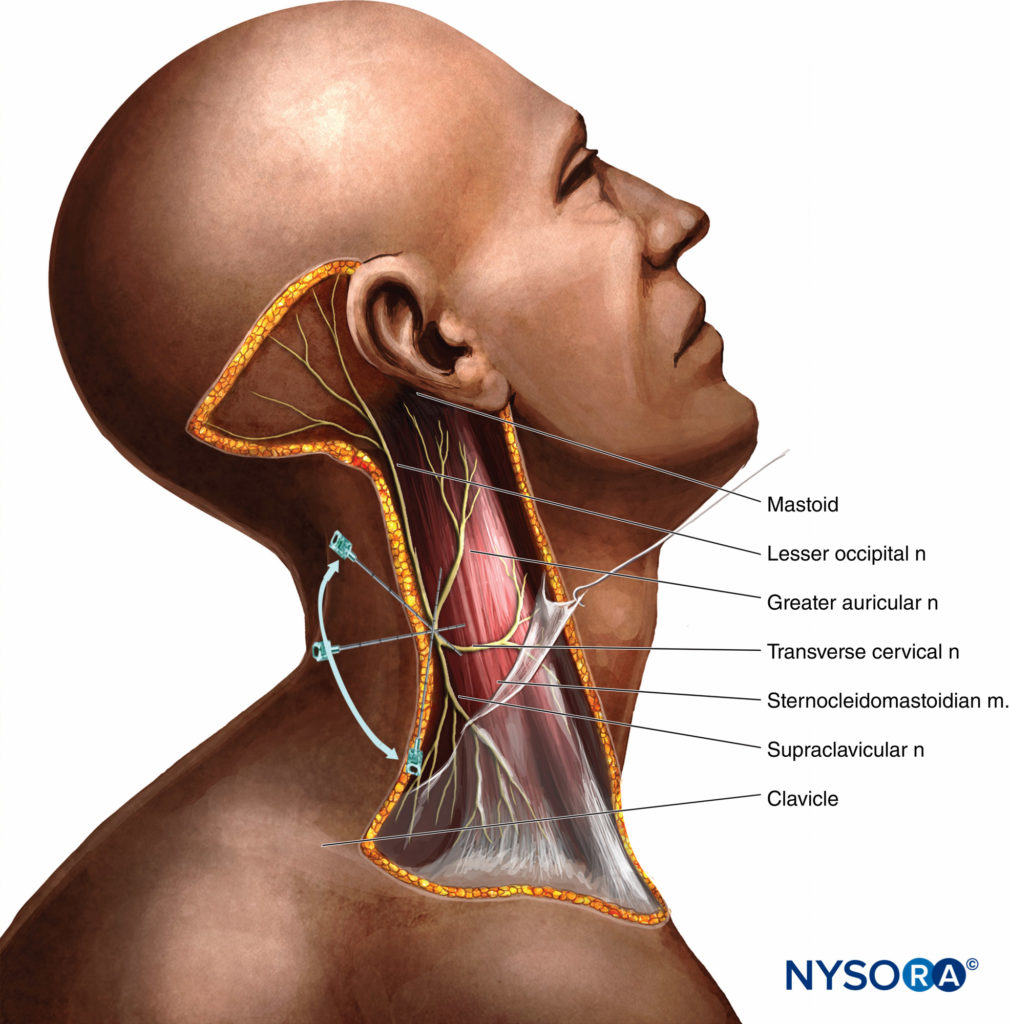
Figure 8. Supraclavicular nerve block. An initial injection of 3 mL local anesthetic is deposited at the midpoint of the sternocleidomastoid muscle, followed by 7 mL injected subcutaneously in a caudad and cephalad direction along the posterior border of the muscle.
Choice of Local Anesthetic
Superficial cervical plexus block requires 10–15 mL of local anesthetic (3–5 mL per each redirection/injection). Since a motor block is not sought with this technique a lower concentration of long-acting local anesthetic is most often used (e.g, 0.2–0.5% ropivacaine or 0.25% bupivacaine). Higher concentration, however, may result in both a greater success rate and a longer duration of block. Table 1 shows the choices of local anesthesia, with onset time and duration of anesthesia and analgesia.
Equipment
A standard regional anesthesia tray is prepared with the following equipment:
- Sterile towels and 4-in. × 4-in. gauze pads
- 20-mL syringe with local anesthetic
- Sterile gloves, marking pen
- A 1.5-in., 25-gauge needle for block infiltration
Learn more about Equipment for Regional Anesthesia.
Technique
Anatomic landmarks and the needle insertion point are marked as described above. After cleansing the skin with an antiseptic solution, a skin wheal is raised at the site of needle insertion using a 25-gauge needle. Using a “fan” technique with superior-inferior needle redirections, the local anesthetic is injected alongside the posterior border of the sternocleidomastoid muscle 2–3 cm below and then above the needle insertion site. The goal is to achieve block of all four major branches of the superficial cervical plexus.
The goal of the injection is to infiltrate the local anesthetic subcutaneously and behind the sternocleidomastoid muscle. Deep needle insertion should be avoided (e.g., >1–2 cm).
Block Dynamics and Perioperative Management
The superficial cervical plexus block is associated with minor patient discomfort, so little or no sedation should be required.
Similar to deep cervical plexus block, the sensory coverage of the neck is complex and a degree of cross-coverage from the cervical plexus branches from the opposite side of the neck should be expected. The onset time for this block is 10–15 minutes; the first sign of the block is decreased sensation in the distribution of the superficial cervical plexus.
Ultrasound guidance can also be used when performing the superficial cervical plexus block, although studies to date have not demonstrated an advantage over a landmark-based technique.
NYSORA Tips
- A subcutaneous midline injection of the local anesthetic extending from the thyroid cartilage distally to the suprasternal notch will also block the branches crossing from the opposite side.
- Superficial cervical plexus can be considered as a “field” block and is very useful for preventing pain from surgical skin retractors on the medial aspect of the neck.
COMPLICATIONS AND HOW TO AVOID THEM
Complications can occur with both deep and superficial cervical plexus blocks (Table 2). Infection, hematoma formation, phrenic nerve block, local anesthetic toxicity, nerve injury, and inadvertent subarachnoid or epidural anesthesia can all occur when performing these blocks. In a large prospective study of 1000 blocks for carotid artery surgery, Davies and colleagues reported only 6 blocks (0.6%) showing evidence of intravascular injection. Other possible complications include transient ischemic attacks either during surgery or in the postoperative period and recurrent laryngeal nerve block. As with other nerve blocks, the risk of complications can be decreased by meticulous technique and attention to detail.
TABLE 2. Complications of cervical plexus block and means to avoid them.
| Infection | • Low risk • A strict aseptic technique is used |
| Hematoma | • Avoid multiple needle insertions, particularly in anticoagulated patients • Keep 5 minutes of steady pressure on the site if the carotid artery is inadvertently punctured |
| Phrenic nerve block | • Phrenic nerve block (diaphragmatic paresis) invariably occurs with a deep cervical plexus block • A deep cervical block should be carefully considered in patients with significant respiratory disease • Bilateral deep cervical block in such patients may be contraindicated • block of the phrenic nerve does not occur after superficial cervical plexus block |
| Local anesthetic toxicity | • Central nervous system toxicity is the most serious consequence of the cervical plexus block • This complication occurs because of the rich vascularity of the neck, including vertebral and carotid artery vessels and is usually caused by an inadvertent intravascular injection of local anesthetic rather than absorption • Careful and frequent aspiration should be performed during the injection |
| Nerve injury | • Local anesthetic should never be injected against resistance or when the patient complains of severe pain on injection |
| Spinal anesthesia | • This complication may occur with injection of a larger volume of local anesthetic inside the dural sleeve that accompanies the nerves of the cervical plexus • It should be noted that a negative aspiration test for CSF does not rule out the possibility of intrathecal spread of local anesthetic • Avoidance of high volume and excessive pressure during injection are the best measures to avoid this complication |
SUMMARY
In summary, cervical plexus blocks have been in clinical use for nearly a century. Although modifications have been made to the approaches first described, the most common approach remains the lateral approach to deep cervical plexus block.
REFERENCES
- Kappis H: Über Leitunganaesthesie am Bauch, Brust, Arm, und Hals durch injection aus Foramen intervertebrale. Munchen Med Wschr 1912;59:794–796.
- Boezaart AP, Koorn R, Rosenquist RW: Paravertebral approach to the brachial plexus: An anatomic improvement in technique. Reg Anesth Pain Med 2003;28:241–244.
- Koorn R, Tenhundfel Fear KM, Miller C, Boezaart A:: The use of cervical paravertebral block as the sole anesthetic for shoulder surgery in a morbid patient: A case report. Reg Anesth Pain Med 2004;29:227–229.
- Borene SC, Rosenquist RW, Koorn R, et al: An indication for con tinuous cervical paravertebral block (posterior approach to the in-terscalene space). Anesth Analg 2003;97:898–900.
- Boezaart AP, Koorn R, Borene S, et al: Continuous brachial plexus block using the posterior approach. Reg Anesth Pain Med 2003;28:70–71.
- Heidenhein L: Operations on the neck. In Braun H (ed): Local Anesthesia, Its Scientific Basis and Practical Use. Philadelphia, PA: Lea & Febiger, 1914, pp 268–269.
- Sherwood-Dunn B: Regional Anesthesia (Victor Pauchet’s Technique). Philadelphia, PA: FA Davis, 1920.
- Winnie AP, Ramamurthy S, Durrani Z, et al: Interscalene cervical plexus block: a single-injection technique. Anesth Analg 1975;54:370–375.
- Todesco J, Williams RT: Anaesthetic management of a patient with a large neck mass. Can J Anaesth 1994;41:157–160.
- Kulkarni RS, Braverman LE, Patwardhan NA: Bilateral cervical plexus block for thyroidectomy and parathyroidectomy in healthy and high risk patients. J Endocrinol Invest 1996;19:714–718.
- Eastcott HH, Pickering GW, Rob CG: Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet 1954;267:994–996.
- Stoneham MD, Knighton JD: Regional anaesthesia for carotid endarterectomy. Br J Anaesth 1999;82:910–919.
- Davies MJ, Silbert BS, Scott DA, et al: Superficial and deep cervical plexus block for carotid artery surgery: a prospective study of 1000 blocks. Reg Anesth Pain Med 1997;22:442–446.
- Stoneburner JM, Nishanian GP, Cukingnan RA, et al: Carotid en-darterectomy using regional anesthesia: a benchmark for stenting. Am Surg 2002;68:1120–1123.
- Harbaugh RE, Pikus HJ: Carotid endarterectomy with regional anes-thesia. Neurosurgery 2001;49:642–645.
- McCleary AJ, Maritati G, Gough MJ: Carotid endarterectomy; local or general anaesthesia? Eur J Vasc Endovasc Surg 2001;22:1–12.
- Melliere D, Desgranges P, Becquemin JP, et al: Surgery of the internal carotid: locoregional or general anesthesia? Ann Chir 2000;125:530–538.
- Stone ME Jr, Kunjummen BJ, Moran JC, et al: Supervised training of general surgery residents in carotid endarterectomy performed on awake patients under regional block is safe and desirable. Am Surg 2000; 66:781–786.
- Knighton JD, Stoneham MD: Carotid endarterectomy. A survey of UK anaesthetic practice. Anaesthesia 2000;55:481–485.
20. Lehot JJ, Durand PG: Anesthesia for carotid endarterectomy. Rev Esp Anestesiol Reanim 2001;48:499–507. - Santamaria G, Britti RD, Tescione M, et al: Comparison between local and general anaesthesia for carotid endarterectomy. A retrospective analysis. Minerva Anestesiol 2004;70:771–778.
- Bowyer MW, Zierold D, Loftus JP, et al: Carotid endarterectomy: a comparison of regional versus general anesthesia in 500 operations. Ann Vasc Surg 2000;14:145–151.
- Papavasiliou AK, Magnadottir HB, Gonda T, et al: Clinical outcomes after carotid endarterectomy: Comparison of the use of regional and general anesthetics. J Neurosurg 2000;92:291–296.
- Stoughton J, Nath RL, Abbott WM: Comparison of simultaneous electroencephalographic and mental status monitoring during carotid endarterectomy with regional anesthesia. J Vasc Surg 1998;28: 1014–1021
- Bonalumi F, Vitiello R, Miglierina L, et al: Carotid endarterectomy under locoregional anesthesia. Ann Ital Chir 1997;68:453–461.
- GALA Trial Collaborative Group: General anaesthesia versus local anaesthesia for carotid surgery (GALA): a multicentre, randomised controlled trial. Lancet 2008;372:2132–2142.
- Vaniyapong T, Chongruksut W, Rerkasem K: Local versus general anaesthesia for carotid endarterectomy. Cochrane Database Syst Rev. 2013; 19:12.
- Brull SJ: Superficial cervical plexus block for pulmonary artery catheter insertion. Crit Care Med 1992;20:1362–1363.
- Pandit JJ, Bree S, Dillon P, et al: A comparison of superficial versus combined (superficial and deep) cervical plexus block for carotid endarterectomy: a prospective, randomized study. Anesth Analg 2000;91: 781–786.
- Stoneham MD, Doyle AR, Knighton JD, et al: Prospective, randomized comparison of deep or superficial cervical plexus block for carotid endarterectomy surgery. Anesthesiology 1998;89:907–912.
- JJ Pandit JJ, Satya-Krishna, Gration P: Superficial or deep cervical plexus block for carotid endarterectomy: a systematic review of complications Br J Anaesth, 99 (2007), pp. 159–169.
- Aunac S, Carlier M, Singelyn F, et al: The analgesic efficacy of bilateral combined superficial and deep cervical plexus block administered before thyroid surgery under general anesthesia. Anesth Analg 2002;95: 746–750.
- Masters RD, Castresana EJ, Castresana MR: Superficial and deep cervical plexus block: Technical considerations. AANA J 1995;63:235–243.
- Dieudonne N, Gomola A, Bonnichon P, et al: Prevention of postoperative pain after thyroid surgery: a double-blind randomized study of bilateral superficial cervical plexus blocks. Anesth Analg 2001;92: 1538–1542.
- Gratz I, Deal E, Larijani GE, et al: The number of injections does not influence absorption of bupivacaine after cervical plexus block for carotid endarterectomy. J Clin Anesth 2005;17:263–266.
- Umbrain VJ, van Gorp VL, Schmedding E, et al: Ropivacaine 3.75 mg/ml, 5 mg/ml, or 7.5 mg/ml for cervical plexus block during carotid endarterectomy. Reg Anesth Pain Med 2004;29:312–316.
- Leoni A, Magrin S, Mascotto G, et al: Cervical plexus anesthesia for carotid endarterectomy: comparison of ropivacaine and mepivacaine. Can J Anaesth 2000;47:185–187.
- Gürkan Y, Taş Z, Toker K, Solak M: Ultrasound guided bilateral cervical plexus block reduces postoperative opioid consumption following thyroid surgery. J Clin Monit Comput. 2015; 29(5):579–584.
- Tran DQ, Dugani S, Finlayson RJ: A randomized comparison between ultrasound-guided and landmark-based superficial cervical plexus block. Reg Anesth Pain Med 2010;35(6):539–543.
- Pandit JJ, McLaren ID, Crider B: Efficacy and safety of the superficial cervical plexus block for carotid endarterectomy. Br J Anaesth 1999; 83:970–972.
- Carling A, Simmonds M: Complications from regional anaesthesia for carotid endarterectomy. Br J Anaesth 2000;84:797–800.
- Emery G, Handley G, Davies MJ, et al: Incidence of phrenic nerve block and hypercapnia in patients undergoing carotid endarterectomy under cervical plexus block. Anaesth Intensive Care 1998;26: 377–381.
- Stoneham MD, Wakefield TW: Acute respiratory distress after deep cervical plexus block. J Cardiothorac Vasc Anesth 1998;12:197–198.
- Castresana MR, Masters RD, Castresana EJ, et al: Incidence and clinical significance of hemidiaphragmatic paresis in patients undergoing carotid endarterectomy during cervical plexus block anesthesia. J Neurosurg Anesthesiol 1994;6:21–23.
- Johnson TR: Transient ischaemic attack during deep cervical plexus block. Br J Anaesth 1999;83:965–967.
- Lawrence PF, Alves JC, Jicha D, et al: Incidence, timing, and causes of cerebral ischemia during carotid endarterectomy with regional anesthesia. J Vasc Surg 1998;27:329–334.
- Harris RJ, Benveniste G: Recurrent laryngeal nerve block in patients undergoing carotid endarterectomy under cervical plexus block. Anaesth Intensive Care 2000;28: 431–433.
- Bergeron P, Benichou H, Dupont M, et al: Carotid surgery under cervical block anesthesia. A simple method of heart and brain protection in high risk patients. Int Angiol 1989;8:70–80.
- Shah DM, Darling RC 3rd, Chang BB, et al: Carotid endarterectomy in awake patients: Its safety, acceptability, and outcome. J Vasc Surg 1994;19:1015–1019.
- Lee KS, Davis CH Jr, McWhorter JM: Low morbidity and mortality of carotid endarterectomy performed with regional anesthesia. J Neurosurg 1988;69:483–487.
- Love A, Hollyoak MA: Carotid endarterectomy and local anaesthesia: reducing the disasters. Cardiovasc Surg 2000;8:429–435.